EXHIBIT 99.2
Published on June 2, 2020
EXHIBIT 99.2

INNOVATING FOR PATIENTS Nasdaq TRVN I May 2020
Forward - Looking Statements To the extent that statements contained in this presentation are not descriptions of historical facts regarding Trevena, Inc . (the “Company” or “we”), they are forward - looking statements reflecting management’s current beliefs and expectations . Forward - looking statements are subject to known and unknown risks, uncertainties, and other factors that may cause our or our industry’s actual results, levels of activity, performance, or achievements to be materially different from those anticipated by such statements . You can identify forward - looking statements by terminology such as “may,” “will,” “should,” “expects,” “plans,” “anticipates,” “believes,” “estimates,” “predicts,” “potential,” “intends,” or “continue,” or the negative of these terms or other comparable terminology . Forward - looking statements contained in this presentation include, but are not limited to, ( i ) statements regarding the timing of anticipated clinical trials for our product candidates ; (ii) the timing of receipt of clinical data for our product candidates ; (iii) our expectations regarding the potential safety, efficacy, or clinical utility of our product candidates ; (iv) the size of patient populations targeted by our product candidates and market adoption of our potential drugs by physicians and patients ; (v) the timing or likelihood of regulatory filings and approvals ; and (vi) our cash needs . Various factors may cause differences between our expectations and actual results, including : unexpected safety or efficacy data, unexpected side effects observed during preclinical studies or in clinical trials ; lower than expected enrollment rates in clinical trials ; changes in expected or existing competition ; uncertainties regarding the regulatory submission and approval process ; changes in the regulatory environment for our drug candidates ; changes in our need for future capital ; unexpected manufacturing or other supply disruptions ; the inability to protect our intellectual property ; and the risk that we become a party to unexpected litigation or other disputes . You should read our filings with the Securities and Exchange Commission, including the Risk Factors set forth in our Annual Report on Form 10 - K and our Quarterly Reports on Form 10 - Q filed with the Securities and Exchange Commission and other filings the Company makes with the Securities and Exchange Commission from time to time , completely and with the understanding that our actual future results may be materially different from what we expect . Except as required by law, we assume no obligation to update these forward - looking statements publicly, or to update the reasons why actual results could differ materially from those anticipated in the forward - looking statements, even if new information becomes available in the future . 2
BOARD OF DIRECTORS Leon O. Moulder , Jr. Chairman Carrie L. Bourdow Julie H. McHugh Scott Braunstein, M.D. Jake R. Nunn Michael R. Dougherty Anne M. Phillips, M.D. Maxine Gowen, Ph.D. Barbara Yanni SENIOR MANAGEMENT Carrie L. Bourdow President & Chief Executive Officer Scott Applebaum SVP, Chief Legal & Compliance Officer Mark A. Demitrack, M.D . SVP, Chief Medical Officer Barry Shin SVP, Chief Financial Officer Robert T. Yoder SVP, Chief Business Officer Trevena’s Experienced Leadership Team 3
Lead asset IV Oliceridine New MOA designed to improve intravenous (IV) moderate - to - severe acute pain management PDUFA date: August 7, 2020 Large market, targeted launch 45M+ US hospital patients; 9M at higher risk for AEs (initial focus) $1 - 1.5B market opportunity for higher - risk patient segment Novel CNS pipeline New mechanisms for acute migraine, opioid use disorder, epilepsy, pain NCEs targeting significant unmet needs NCE for COVID - 19 Novel MOA to treat COVID - 19 acute lung injury POC study sponsored by Imperial College London Solid financial position $28.1M in cash as of 3/31/2020 Funds operations into Q1 2021 Trevena: Innovative CNS Company 4 MOA = Mechanism of Action; PDUFA = Prescription Drug User Fee Act; NCE = New Chemical Entity
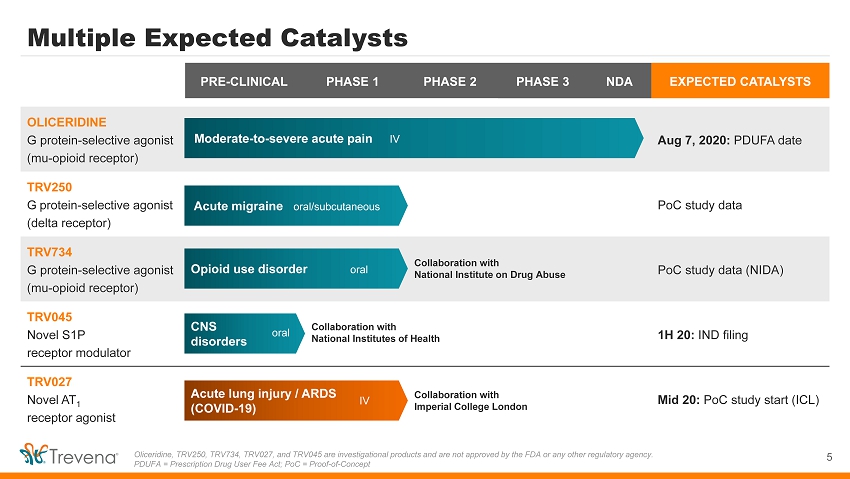
PRE - CLINICAL PHASE 1 PHASE 2 PHASE 3 NDA EXPECTED CATALYSTS OLICERIDINE G protein - selective agonist (mu - opioid receptor) Aug 7, 2020: PDUFA date TRV250 G protein - selective agonist (delta receptor) PoC study data TRV734 G protein - selective agonist (mu - opioid receptor) PoC study data (NIDA) TRV045 Novel S1P receptor modulator 1H 20: IND filing TRV027 Novel AT 1 receptor agonist Mid 20: PoC study start (ICL) Multiple Expected Catalysts 5 Oliceridine, TRV250, TRV734, TRV027, and TRV045 are investigational products and are not approved by the FDA or any other reg ula tory agency. PDUFA = Prescription Drug User Fee Act; PoC = Proof - of - Concept Moderate - to - severe acute pain IV Acute migraine oral/subcutaneous Collaboration with National Institute on Drug Abuse Opioid use disorder oral CNS disorders Collaboration with National Institutes of Health Acute lung injury / ARDS (COVID - 19) oral IV Collaboration with Imperial College London
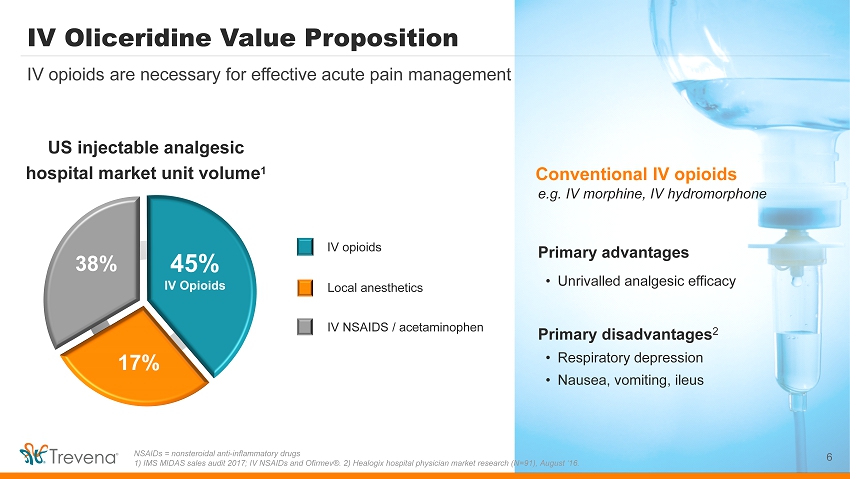
IV Oliceridine Value Proposition 6 IV opioids are necessary for effective acute pain management NSAIDs = nonsteroidal anti - inflammatory drugs 1) IMS MIDAS sales audit 2017; IV NSAIDs and Ofirmev ®. 2) Healogix hospital physician market research (N=91), August ‘16. e.g. IV morphine, IV hydromorphone • Unrivalled analgesic efficacy • Respiratory depression • Nausea, vomiting, ileus IV NSAIDS / acetaminophen Conventional IV opioids US injectable analgesic hospital market unit volume 1 IV opioids 45% IV Opioids 17% 38% Local anesthetics Primary advantages Primary disadvantages 2
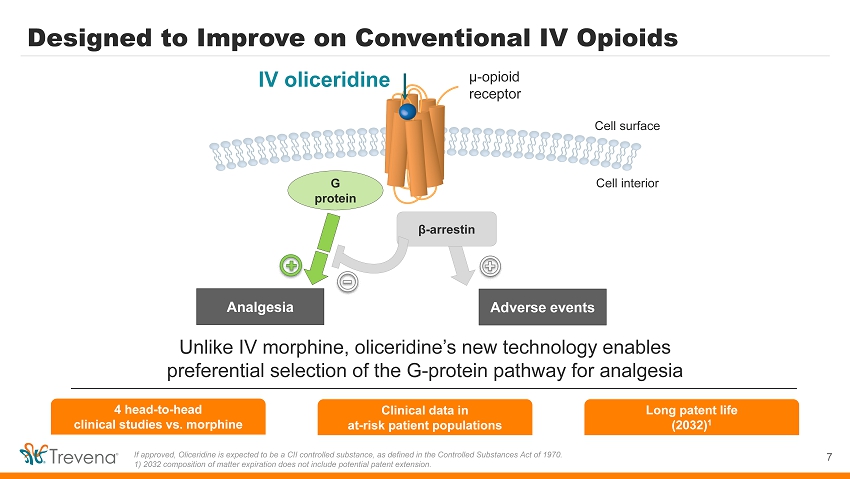
4 head - to - head clinical studies vs. morphine Designed to Improve on Conventional IV Opioids 7 If approved, Oliceridine is expected to be a CII controlled substance, as defined in the Controlled Substances Act of 1970. 1) 2032 composition of matter expiration does not include potential patent extension. Unlike IV morphine, oliceridine’s new technology enables preferential selection of the G - protein pathway for analgesia Analgesia Adverse events IV oliceridine µ - opioid receptor Cell surface Cell interior β - arrestin G protein Clinical data in at - risk patient populations Long patent life (2032) 1
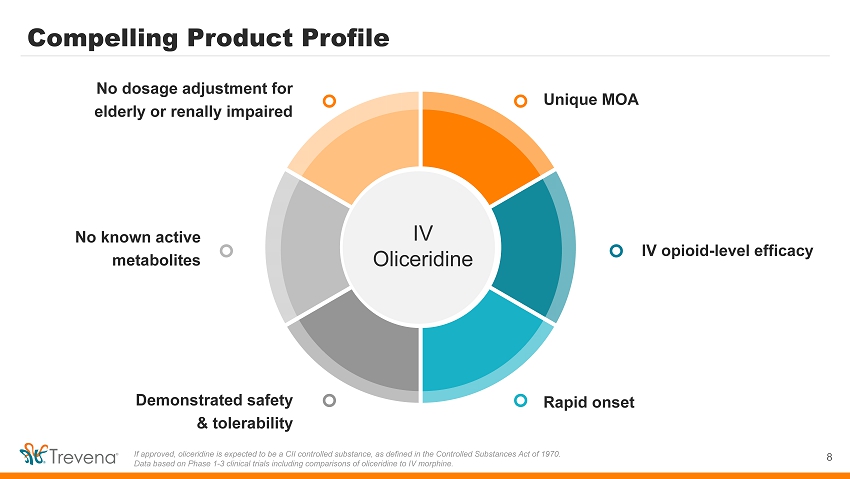
Compelling Product Profile 8 If approved, oliceridine is expected to be a CII controlled substance, as defined in the Controlled Substances Act of 1970. Data based on Phase 1 - 3 clinical trials including comparisons of oliceridine to IV morphine. Unique MOA IV opioid - level efficacy Rapid onset No dosage adjustment for elderly or renally impaired No known active metabolites Demonstrated safety & tolerability IV Oliceridine
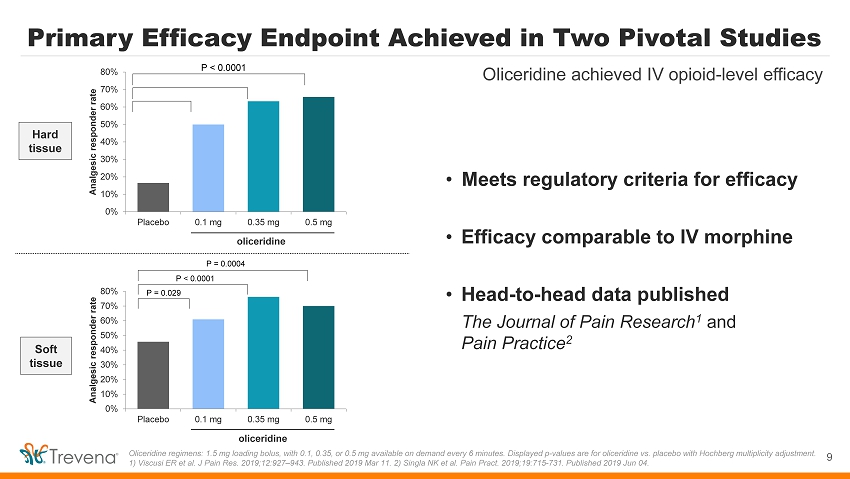
Soft tissue Primary Efficacy Endpoint Achieved in Two Pivotal Studies Oliceridine regimens: 1.5 mg loading bolus, with 0.1, 0.35, or 0.5 mg available on demand every 6 minutes. Displayed p - values ar e for oliceridine vs. placebo with Hochberg multiplicity adjustment. 1) Viscusi ER et al. J Pain Res. 2019;12:927 – 943. Published 2019 Mar 11. 2) Singla NK et al. Pain Pract . 2019;19:715 - 731. Published 2019 Jun 04. 9 Oliceridine achieved IV opioid - level efficacy Hard tissue • Meets regulatory criteria for efficacy • Efficacy comparable to IV morphine • Head - to - head data published The Journal of Pain Research 1 and Pain Practice 2 0% 10% 20% 30% 40% 50% 60% 70% 80% Placebo 0.1 mg 0.35 mg 0.5 mg Analgesic responder rate oliceridine P < 0.0001 0% 10% 20% 30% 40% 50% 60% 70% 80% Placebo 0.1 mg 0.35 mg 0.5 mg Analgesic responder rate oliceridine P = 0.029 P < 0.0001 P = 0.0004
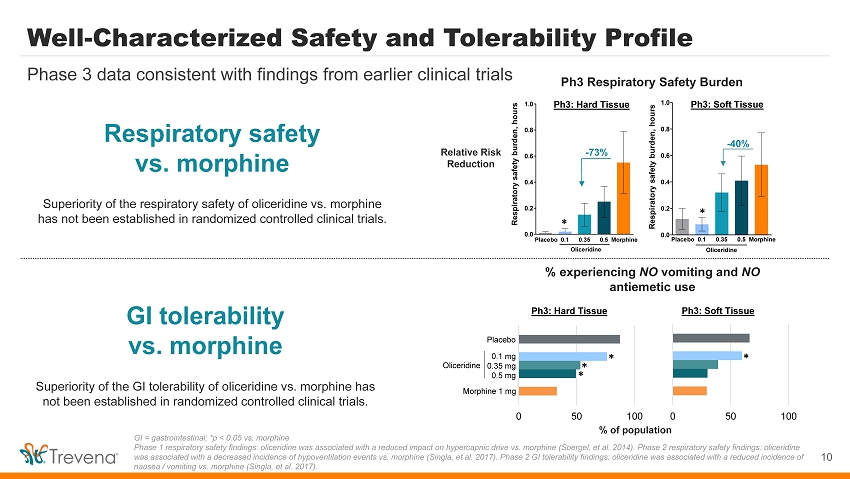
0.0 0.2 0.4 0.6 0.8 1.0 Respiratory safety burden, hours Placebo 0.1 0.35 0.5 Morphine Oliceridine Placebo 0.1 0.35 0.5 Morphine 0.0 0.2 0.4 0.6 0.8 1.0 Respiratory safety burden, hours Oliceridine - 73% - 40% Ph3 Respiratory Safety Burden Relative Risk Reduction Ph3: Hard Tissue Ph3: Soft Tissue Well - Characterized Safety and Tolerability Profile 10 Phase 3 data consistent with findings from earlier clinical trials GI = gastrointestinal; *p < 0.05 vs. morphine Phase 1 respiratory safety findings: oliceridine was associated with a reduced impact on hypercapnic drive vs. morphine (Soer gel , et al. 2014). Phase 2 respiratory safety findings: oliceridine was associated with a decreased incidence of hypoventilation events vs. morphine (Singla, et al. 2017). Phase 2 GI tolerabili ty findings: oliceridine was associated with a reduced incidence of nausea / vomiting vs. morphine (Singla, et al. 2017). Respiratory safety vs. morphine GI tolerability vs. morphine % experiencing NO vomiting and NO antiemetic use % of population 0 50 100 Ph3: Hard Tissue Placebo Morphine 1 mg Oliceridine 0.1 mg 0.35 mg 0.5 mg * * * 0 50 100 Ph3: Soft Tissue * Superiority of the respiratory safety of oliceridine vs. morphine has not been established in randomized controlled clinical trials. Superiority of the GI tolerability of oliceridine vs. morphine has not been established in randomized controlled clinical trials. * *
Unique and Differentiated PK Profile 11 PK = pharmacokinetic. Icons made by Freepik from www.flaticon.com IV oliceridine demonstrates: Fast onset (<5 min) + ~3 - hour duration Attractive for ER, hospital floor, and surgery centers No known active metabolites Simplifies dosing for predictable pain control New option for at - risk patients No dosage adjustments (elderly/ renally impaired)
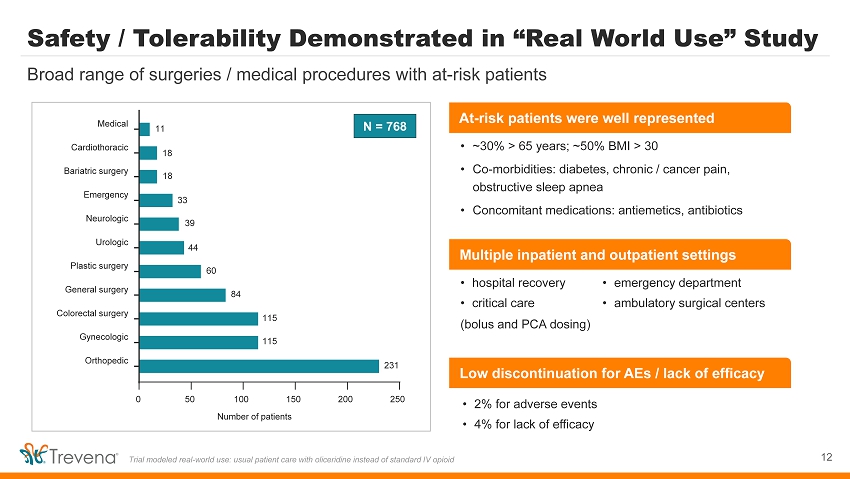
Safety / Tolerability Demonstrated in “Real World Use” Study 12 Broad range of surgeries / medical procedures with at - risk patients Trial modeled real - world use: usual patient care with oliceridine instead of standard IV opioid 0 50 100 150 200 250 Orthopedic Gynecologic Colorectal surgery General surgery Plastic surgery Urologic Neurologic Emergency Bariatric surgery Cardiothoracic Medical Number of patients 11 18 18 33 39 44 60 84 115 115 231 N = 768 • 2% for adverse events • 4% for lack of efficacy • hospital recovery • critical care • emergency department • ambulatory surgical centers (bolus and PCA dosing) • ~30% > 65 years; ~50% BMI > 30 • Co - morbidities: diabetes, chronic / cancer pain, obstructive sleep apnea • Concomitant medications: antiemetics, antibiotics Multiple inpatient and outpatient settings At - risk patients were well represented Low discontinuation for AEs / lack of efficacy
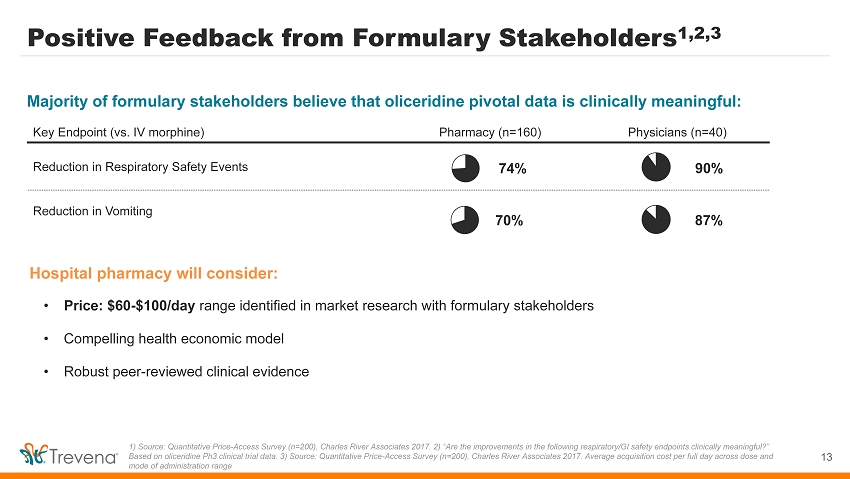
Positive Feedback from Formulary Stakeholders 1,2,3 13 1) Source: Quantitative Price - Access Survey (n=200), Charles River Associates 2017. 2) “Are the improvements in the following re spiratory/GI safety endpoints clinically meaningful?” Based on oliceridine Ph3 clinical trial data. 3) Source: Quantitative Price - Access Survey (n=200), Charles River Associates 2017 . Average acquisition cost per full day across dose and mode of administration range • Price: $60 - $100/day range identified in market research with formulary stakeholders • Compelling health economic model • Robust peer - reviewed clinical evidence Hospital pharmacy will consider: Key Endpoint (vs. IV morphine) Pharmacy (n=160) Physicians (n=40) Reduction in Respiratory Safety Events Reduction in Vomiting Majority of formulary stakeholders believe that oliceridine pivotal data is clinically meaningful: 74% 90% 70% 87%
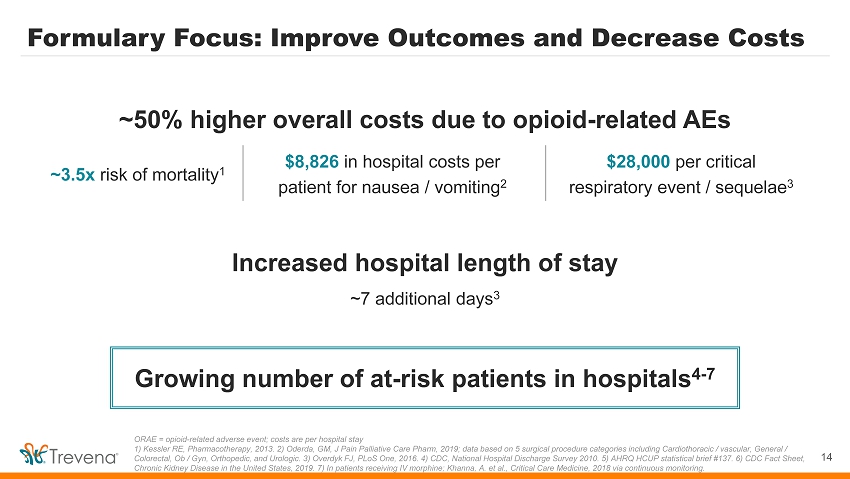
Formulary Focus: Improve Outcomes and Decrease Costs 14 ORAE = opioid - related adverse event; costs are per hospital stay 1) Kessler RE, Pharmacotherapy, 2013. 2) Oderda , GM, J Pain Palliative Care Pharm, 2019; data based on 5 surgical procedure categories including Cardiothoracic / vascular, Gen eral / Colorectal, Ob / Gyn, Orthopedic, and Urologic. 3) Overdyk FJ, PLoS One, 2016. 4) CDC, National Hospital Discharge Survey 2010. 5) AHRQ HCUP statistical brief #137. 6) CDC Fact Sheet, Chronic Kidney Disease in the United States, 2019. 7) In patients receiving IV morphine; Khanna, A. et al., Critical Care Medicine, 2018 via continuous monitoring. Growing number of at - risk patients in hospitals 4 - 7 ~3.5x risk of mortality 1 ~50% higher overall costs due to opioid - related AEs $8,826 in hospital costs per patient for nausea / vomiting 2 $28,000 per critical respiratory event / sequelae 3 Increased hospital length of stay ~7 additional days 3
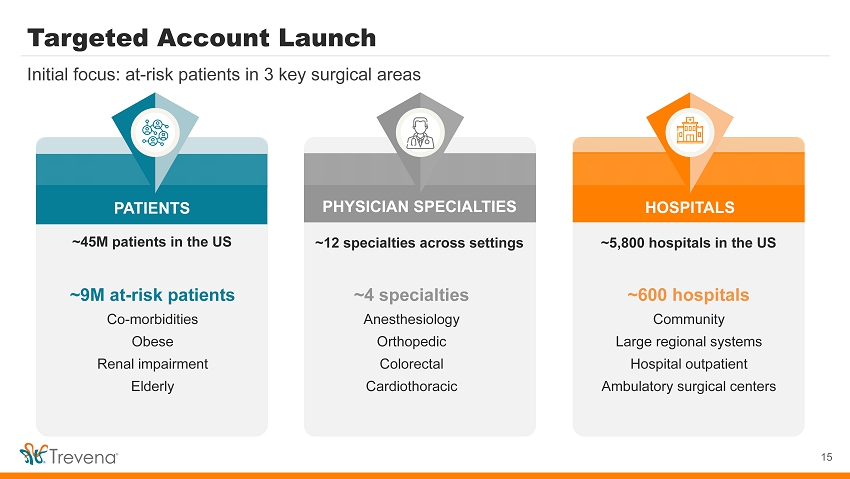
PATIENTS HOSPITALS Targeted Account Launch 15 Initial focus: at - risk patients in 3 key surgical areas ~5,800 hospitals in the US ~600 hospitals Community Large regional systems Hospital outpatient Ambulatory surgical centers ~9M at - risk patients Co - morbidities Obese Renal impa irment Elderly PHYSICIAN SPECIALTIES ~12 specialties across settings ~45M patients in the US ~4 specialties Anesthesiology Orthopedic Colorectal Cardiothoracic
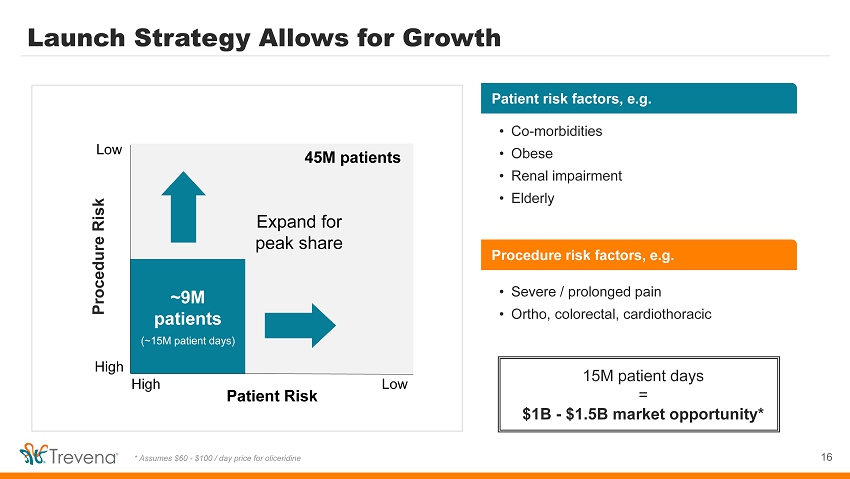
Procedure risk factors, e.g. Procedure Risk Patient Risk High High Low Launch Strategy Allows for Growth 16 * Assumes $60 - $100 / day price for oliceridine Low Initial launch focus Expand for peak share • Severe / prolonged pain • Ortho, colorectal, cardiothoracic • Co - morbidities • Obese • Renal impairment • Elderly 45M patients ~9M patients (~15M patient days) Patient risk factors, e.g. 15M patient days = $1B - $1.5B market opportunity*
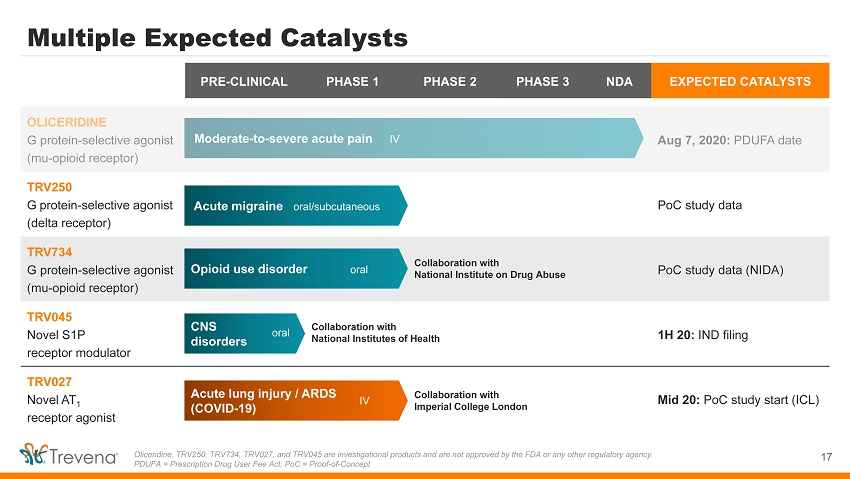
PRE - CLINICAL PHASE 1 PHASE 2 PHASE 3 NDA EXPECTED CATALYSTS OLICERIDINE G protein - selective agonist (mu - opioid receptor) Aug 7, 2020: PDUFA date TRV250 G protein - selective agonist (delta receptor) PoC study data TRV734 G protein - selective agonist (mu - opioid receptor) PoC study data (NIDA) TRV045 Novel S1P receptor modulator 1H 20: IND filing TRV027 Novel AT 1 receptor agonist Mid 20: PoC study start (ICL) Multiple Expected Catalysts 17 Oliceridine, TRV250, TRV734, TRV027, and TRV045 are investigational products and are not approved by the FDA or any other reg ula tory agency. PDUFA = Prescription Drug User Fee Act; PoC = Proof - of - Concept Moderate - to - severe acute pain IV Acute migraine oral/subcutaneous Collaboration with National Institute on Drug Abuse Opioid use disorder oral CNS disorders Collaboration with National Institutes of Health Acute lung injury / ARDS (COVID - 19) oral IV Collaboration with Imperial College London
Migraine Represents A Large Market Opportunity 18 Total migraine drug market = ~$3.5B All data from Decision Resources, Pharmacor migraine market landscape and forecast 2018. 1) Moven et al., J Neurol Neurosurg Psychiatry, 2016. Icons made by Freepik from www.flaticon.com 650M migraines treated each year 1.2M ER visits due to migraines 20 - 30% of migraine sufferers do not respond to / cannot tolerate the market - leading triptan drug class An estimated 50% of migraineurs also suffer from anxiety 1 Every year in the US:
TRV250: New MOA for Acute Treatment of Migraine 19 Delta receptor: Untapped potential in CNS space Play important role in regulation of pain, mood, and anxiety Acute migraine proof - of - concept study initiated Delta receptors have unique distribution throughout the brain • Validated biomarker model (NTG infusion) • Test dose: 20 mg subcutaneous TRV250 vs. placebo (n=~120 migraineurs) • Primary outcome: reduction of sustained NTG - induced headaches • Secondary outcomes: reduction of symptomatic anxiety, general safety
TRV734: Maintenance Therapy for Opioid Use Disorder 20 Selective agonism at µ receptor: Potential for improved tolerability 1) Center for Behavioral Health Statistics and Quality. 2) NIDA data on file. Ongoing collaboration with National Institute on Drug Abuse (NIDA) >2.5M people in U.S. suffer from opioid use disorder 1 • Nonclinical evidence of improved tolerability with TRV734 • NIDA study demonstrated reduced drug - seeking behavior in animal model of relapse 2 • Current therapies not well tolerated, can hinder patient adherence NIDA - funded proof - of - concept patient study initiated
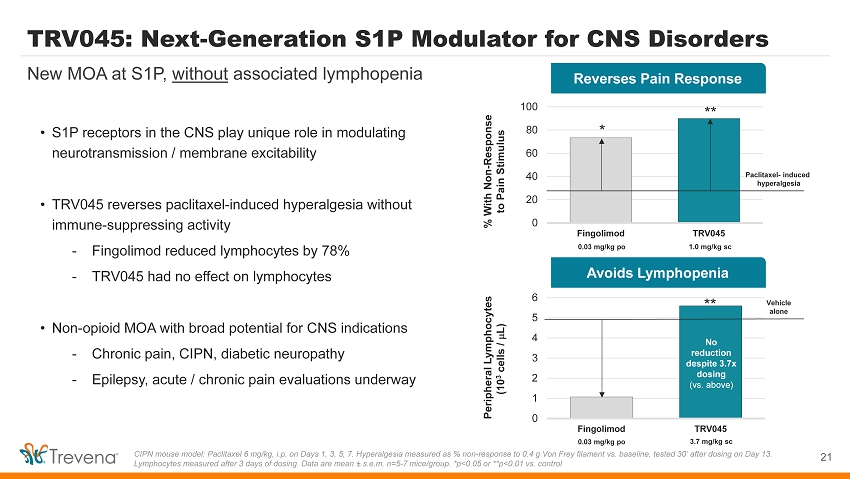
Avoids Lymphopenia Reverses Pain Response TRV045: Next - Generation S1P Modulator for CNS Disorders 0 20 40 60 80 100 Fingolimod TRV045 21 New MOA at S1P, without associated lymphopenia CIPN mouse model: Paclitaxel 6 mg/kg, i.p. on Days 1, 3, 5, 7. Hyperalgesia measured as % non - response to 0.4 g Von Frey filament vs. baseline, tested 30’ after dosing on Day 13. Lymphocytes measured after 3 days of dosing. Data are mean s.e.m. n=5 - 7 mice/group. *p<0.05 or **p<0.01 vs. control • S1P receptors in the CNS play unique role in modulating neurotransmission / membrane excitability • TRV045 reverses paclitaxel - induced hyperalgesia without immune - suppressing activity - Fingolimod reduced lymphocytes by 78% - TRV045 had no effect on lymphocytes • Non - opioid MOA with broad potential for CNS indications - Chronic pain, CIPN, diabetic neuropathy - Epilepsy, acute / chronic pain evaluations underway 0 1 2 3 4 5 6 Fingolimod TRV045 Peripheral Lymphocytes (10 3 cells / m L) % With Non - Response to Pain Stimulus 0.03 mg/kg po 1.0 mg/kg sc 0.03 mg/kg po 3.7 mg/kg sc Paclitaxel - induced hyperalgesia Vehicle alone No reduction despite 3.7x dosing (vs. above) ** * **
TRV027 NCE targeting the AT 1 receptor in COVID - 19 22
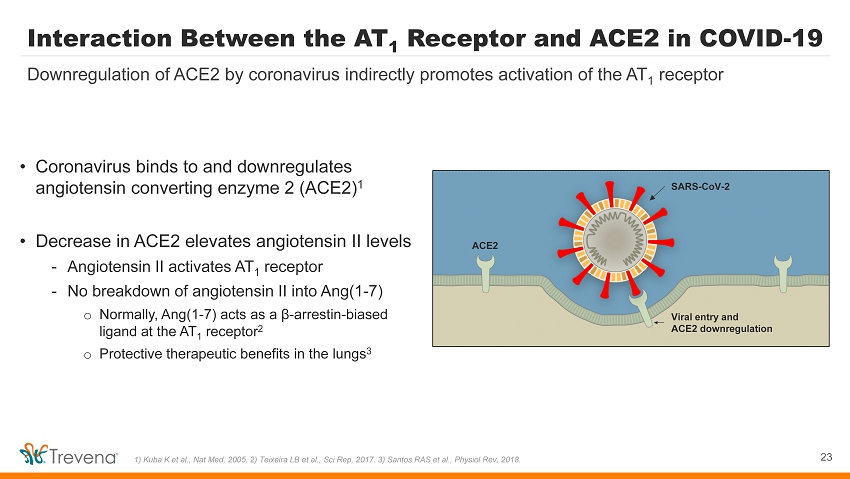
Interaction Between the AT 1 Receptor and ACE2 in COVID - 19 • Coronavirus binds to and downregulates angiotensin converting enzyme 2 (ACE2) 1 • Decrease in ACE2 elevates angiotensin II levels - Angiotensin II activates AT 1 receptor - No breakdown of angiotensin II into Ang(1 - 7) o Normally, Ang(1 - 7) acts as a β - arrestin - biased ligand at the AT 1 receptor 2 o Protective therapeutic benefits in the lungs 3 23 Downregulation of ACE2 by coronavirus indirectly promotes activation of the AT 1 receptor 1) Kuba K et al., Nat Med, 2005. 2) Teixeira LB et al., Sci Rep, 2017. 3) Santos RAS et al., Physiol Rev, 2018. SARS - CoV - 2 ACE2 Viral entry and ACE2 downregulation
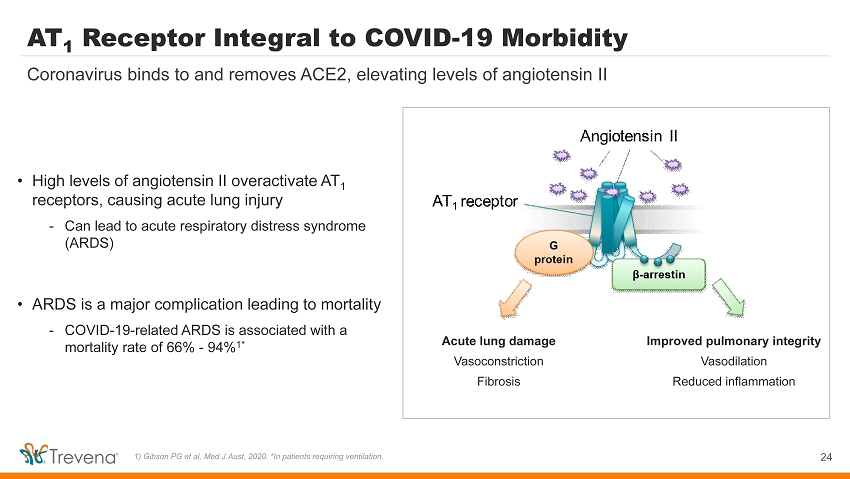
AT 1 Receptor Integral to COVID - 19 Morbidity Acute lung damage Vasoconstriction Fibrosis 24 Coronavirus binds to and removes ACE2, elevating levels of angiotensin II 1) Gibson PG et al, Med J Aust, 2020. *In patients requiring ventilation. Improved pulmonary integrity Vasodilation Reduced inflammation • High levels of angiotensin II overactivate AT 1 receptors, causing acute lung injury - Can lead to acute respiratory distress syndrome (ARDS) • ARDS is a major complication leading to mortality - COVID - 19 - related ARDS is associated with a mortality rate of 66% - 94% 1*
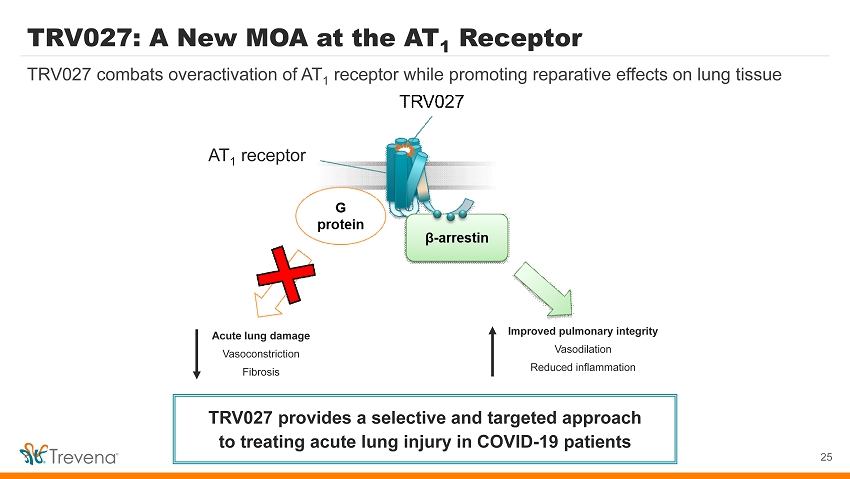
TRV027: A New MOA at the AT 1 Receptor 25 TRV027 combats overactivation of AT 1 receptor while promoting reparative effects on lung tissue TRV027 provides a selective and targeted approach to treating acute lung injury in COVID - 19 patients Acute lung damage Vasoconstriction Fibrosis Improved pulmonary integrity Vasodilation Reduced inflammation AT 1 receptor
TRV027 is Ready to Enter Clinical Testing 26 Safety / tolerability has been established in large patient population • Advanced through Phase 2b for acute heart failure • Studied in ~700 individuals • Well - characterized pharmacology • No significant safety issues during clinical trials TRV027 clinical development history
COVID - 19 Study - Imperial College London • Randomized, double - blind, placebo - controlled proof - of - concept study • N = ~60 (30 per arm) COVID - 19 patients - Hospitalized, non - ventilated - ≥65 years old • IV infusion of placebo or TRV027 for 7 days 27 Investigate effect of TRV027 on pathways that contribute to COVID - 19 pathology Primary endpoint: Coagulation biomarker (predictor of COVID - 19 mortality) • Indicator of TRV027’s effect on health outcomes associated with increased mortality in COVID - 19
Lead asset IV Oliceridine New MOA designed to improve intravenous (IV) moderate - to - severe acute pain management PDUFA date: August 7, 2020 Large market, targeted launch 45M+ US hospital patients; 9M at higher risk for AEs (initial focus) $1 - 1.5B market opportunity for higher - risk patient segment Novel CNS pipeline New mechanisms for acute migraine, opioid use disorder, epilepsy, pain NCEs targeting significant unmet needs NCE for COVID - 19 Novel MOA to treat COVID - 19 acute lung injury POC study sponsored by Imperial College London Solid financial position $28.1M in cash as of 3/31/2020 Funds operations into Q1 2021 Trevena: Innovative CNS Company 28 MOA = Mechanism of Action; PDUFA = Prescription Drug User Fee Act; NCE = New Chemical Entity

APPENDIX 29
NDA Resubmission Considered Complete NDA = New Drug Application 30 Completed healthy volunteer QT study Confirmed safety database supports maximum daily dose of 27 mg Validated bioassay and confirmed levels of inactive metabolite (‘9662) Completed drug product validation reports • No accumulation of effect through 24 hrs despite repeated dosing • No categorical QTc outliers with ∆ > 60 ms or > 500 ms absolute PDUFA date: August 7, 2020
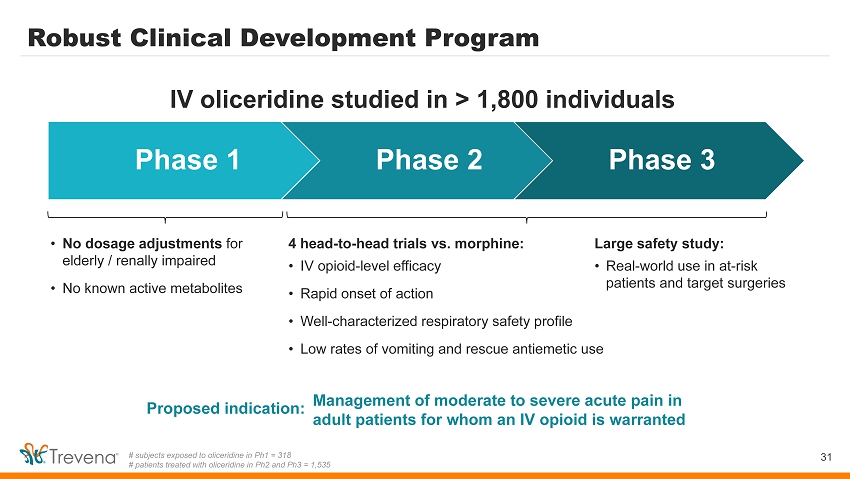
• No dosage adjustments for elderly / renally impaired • No known active metabolites Robust Clinical Development Program 31 # subjects exposed to oliceridine in Ph1 = 318 # patients treated with oliceridine in Ph2 and Ph3 = 1,535 Phase 1 Phase 2 Phase 3 4 head - to - head trials vs. morphine: • IV opioid - level efficacy • Rapid onset of action • Well - characterized respiratory safety profile • Low rates of vomiting and rescue antiemetic use IV oliceridine studied in > 1,800 individuals Management of moderate to severe acute pain in adult patients for whom an IV opioid is warranted Proposed indication: Large safety study: • Real - world use in at - risk patients and target surgeries
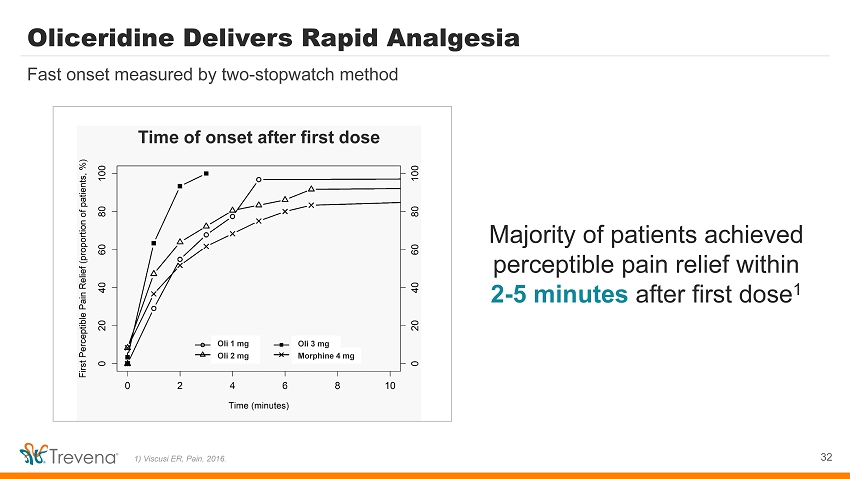
Oli 2 mg Morphine 4 mg Oli 1 mg Oli 3 mg Oliceridine Delivers Rapid Analgesia 32 Fast onset measured by two - stopwatch method Majority of patients achieved perceptible pain relief within 2 - 5 minutes after first dose 1 Time of onset after first dose 1) Viscusi ER, Pain, 2016.
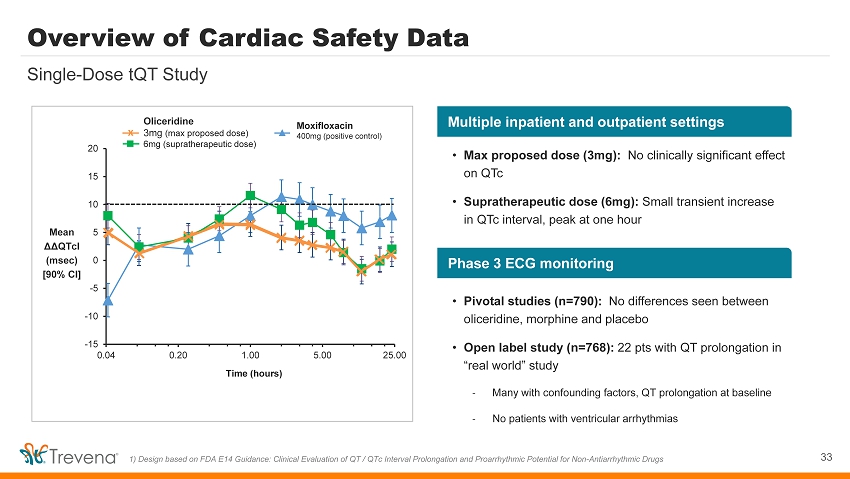
-15 -10 -5 0 5 10 15 20 0.04 0.20 1.00 5.00 25.00 Time (hours) Moxifloxacin 400mg (positive control) Overview of Cardiac Safety Data 33 Single - Dose tQT Study Single - dose Phase 1 tQT study 1 1) Design based on FDA E14 Guidance: Clinical Evaluation of QT / QTc Interval Prolongation and Proarrhythmic Potential for No n - A ntiarrhythmic Drugs Oliceridine 3mg (max proposed dose) 6mg (supratherapeutic dose) x Mean ΔΔ QTcI ( msec ) [90% CI] Multiple inpatient and outpatient settings Phase 3 ECG monitoring • Max proposed dose (3mg): No clinically significant effect on QTc • Supratherapeutic dose (6mg): Small transient increase in QTc interval, peak at one hour • Pivotal studies (n=790): No differences seen between oliceridine, morphine and placebo • Open label study (n=768): 22 pts with QT prolongation in “real world” study - Many with confounding factors, QT prolongation at baseline - No patients with ventricular arrhythmias
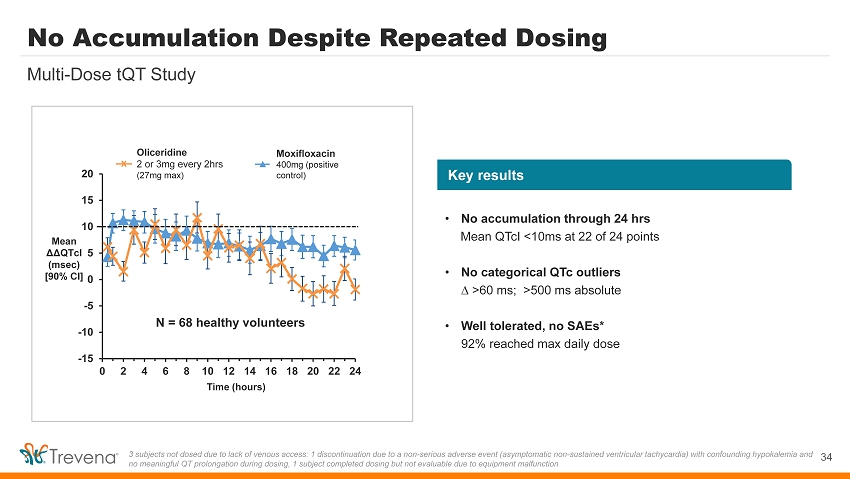
-15 -10 -5 0 5 10 15 20 0 2 4 6 8 10 12 14 16 18 20 22 24 Mean ΔΔ QTcI ( msec ) [90% CI] No Accumulation Despite Repeated Dosing 34 Multi - Dose tQT Study 3 subjects not dosed due to lack of venous access: 1 discontinuation due to a non - serious adverse event (asymptomatic non - sustai ned ventricular tachycardia) with confounding hypokalemia and no meaningful QT prolongation during dosing, 1 subject completed dosing but not evaluable due to equipment malfunction Oliceridine 2 or 3mg every 2hrs (27mg max) x Moxifloxacin 400mg (positive control) Time (hours) N = 68 healthy volunteers Key results • No accumulation through 24 hrs Mean QTcI <10ms at 22 of 24 points • No categorical QTc outliers ∆ >60 ms ; >500 ms absolute • Well tolerated, no SAEs* 92% reached max daily dose
Comprehensive Data Available at Launch 35 Will support future commercialization and hospital formulary uptake *Expected to be published at time of approval / launch • First - in - class new mechanism of action • Fast, effective IV opioid - level pain relief • Clinical data in at - risk patients / targeted surgeries • Published head - to - head trials vs. IV morphine • Published data in at - risk patients & target surgeries • Published health economic / cost offset data* Health Care Practitioners (HCPs) Hospital Formulary Committees
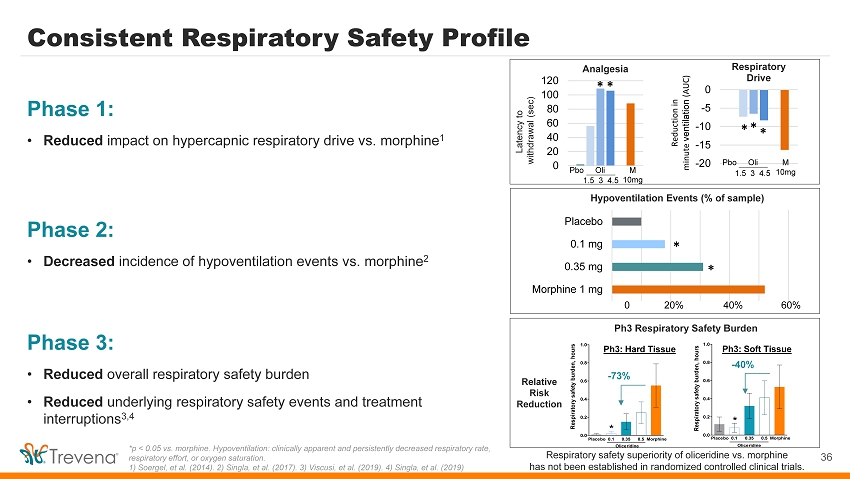
1.5 3 4.5 Respiratory safety superiority of oliceridine vs. morphine has not been established in randomized controlled clinical trials. Consistent Respiratory Safety Profile Phase 1: • Reduced impact on hypercapnic respiratory drive vs. morphine 1 36 *p < 0.05 vs. morphine. Hypoventilation: clinically apparent and persistently decreased respiratory rate, respiratory effort, or oxygen saturation. 1) Soergel, et al. (2014). 2) Singla, et al. (2017). 3) Viscusi, et al. (2019). 4) Singla, et al. (2019) Hypoventilation Events (% of sample) Morphine 1 mg 0.35 mg 0.1 mg Placebo * * 0 20% 40% 60% 0 20 40 60 80 100 120 Analgesia Pbo 1.5 3 4.5 M 10mg Latency to withdrawal (sec) * * -20 -15 -10 -5 0 Respiratory Drive Reduction in minute ventilation (AUC) * * * Oli Phase 2: • Decreased incidence of hypoventilation events vs. morphine 2 Phase 3: • Reduced overall respiratory safety burden • Reduced underlying respiratory safety events and treatment interruptions 3,4 0.0 0.2 0.4 0.6 0.8 1.0 Respiratory safety burden, hours Placebo 0.1 0.35 0.5 Morphine Oliceridine * - 73% Placebo 0.1 0.35 0.5 Morphine 0.0 0.2 0.4 0.6 0.8 1.0 Respiratory safety burden, hours Oliceridine * - 40% Ph3 Respiratory Safety Burden Relative Risk Reduction Ph3: Hard Tissue Ph3: Soft Tissue Pbo M 10mg Oli
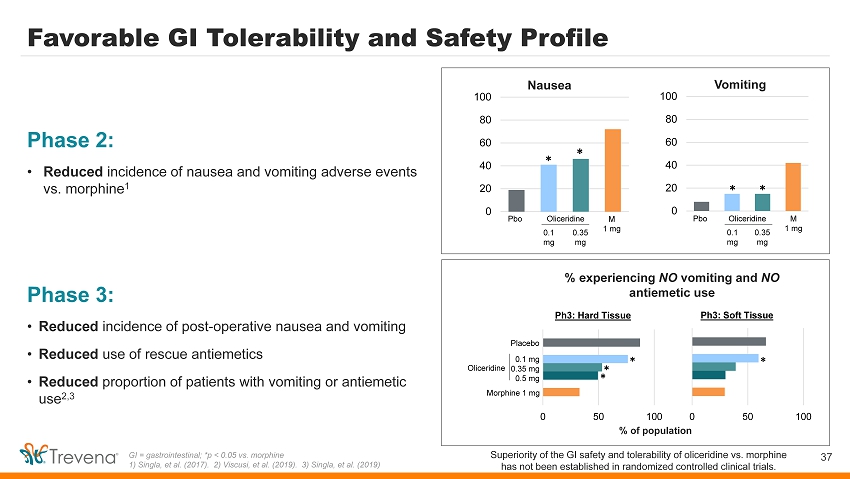
Superiority of the GI safety and tolerability of oliceridine vs. morphine has not been established in randomized controlled clinical trials. Favorable GI Tolerability and Safety Profile Phase 2: • Reduced incidence of nausea and vomiting adverse events vs. morphine 1 37 GI = gastrointestinal; *p < 0.05 vs. morphine 1) Singla, et al. (2017). 2) Viscusi, et al. (2019). 3) Singla, et al. (2019) 0 20 40 60 80 100 Oliceridine 0 20 40 60 80 100 Oliceridine 0.1 mg 0.35 mg 0.1 mg 0.35 mg Nausea Vomiting Pbo M 1 mg Pbo M 1 mg * * * * Phase 3: • Reduced incidence of post - operative nausea and vomiting • Reduced use of rescue antiemetics • Reduced proportion of patients with vomiting or antiemetic use 2,3 % experiencing NO vomiting and NO antiemetic use % of population 0 50 100 Ph3: Hard Tissue Placebo Morphine 1 mg Oliceridine 0.1 mg 0.35 mg 0.5 mg * * * 0 50 100 Ph3: Soft Tissue *
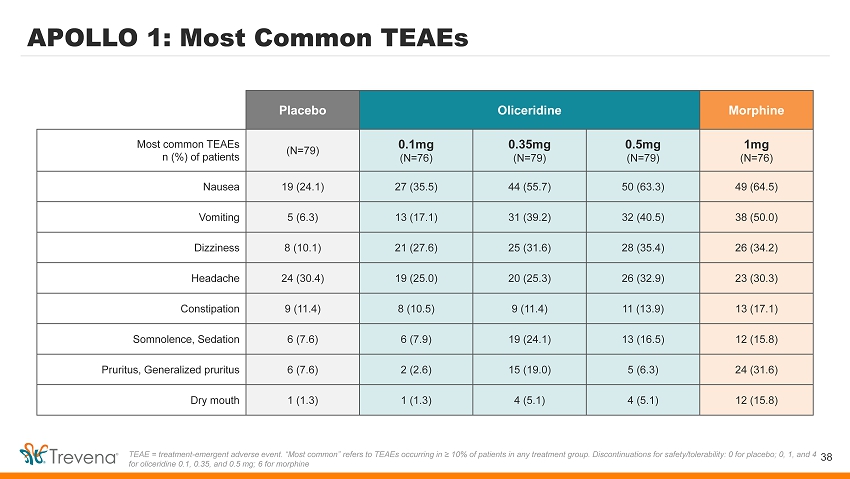
APOLLO 1: Most Common TEAEs 38 TEAE = treatment - emergent adverse event. “Most common” refers to TEAEs occurring in ≥ 10% of patients in any treatment group. Di scontinuations for safety/tolerability: 0 for placebo; 0, 1, and 4 for oliceridine 0.1, 0.35, and 0.5 mg; 6 for morphine Placebo Oliceridine Morphine Most common TEAEs n (%) of patients (N=79) 0.1mg (N=76) 0.35mg (N=79) 0.5mg (N=79) 1mg (N=76) Nausea 19 (24.1) 27 (35.5) 44 (55.7) 50 (63.3) 49 (64.5) Vomiting 5 (6.3) 13 (17.1) 31 (39.2) 32 (40.5) 38 (50.0) Dizziness 8 (10.1) 21 (27.6) 25 (31.6) 28 (35.4) 26 (34.2) Headache 24 (30.4) 19 (25.0) 20 (25.3) 26 (32.9) 23 (30.3) Constipation 9 (11.4) 8 (10.5) 9 (11.4) 11 (13.9) 13 (17.1) Somnolence, Sedation 6 (7.6) 6 (7.9) 19 (24.1) 13 (16.5) 12 (15.8) Pruritus, G eneralized pruritus 6 (7.6) 2 (2.6) 15 (19.0) 5 (6.3) 24 (31.6) Dry mouth 1 (1.3) 1 (1.3) 4 (5.1) 4 (5.1) 12 (15.8)
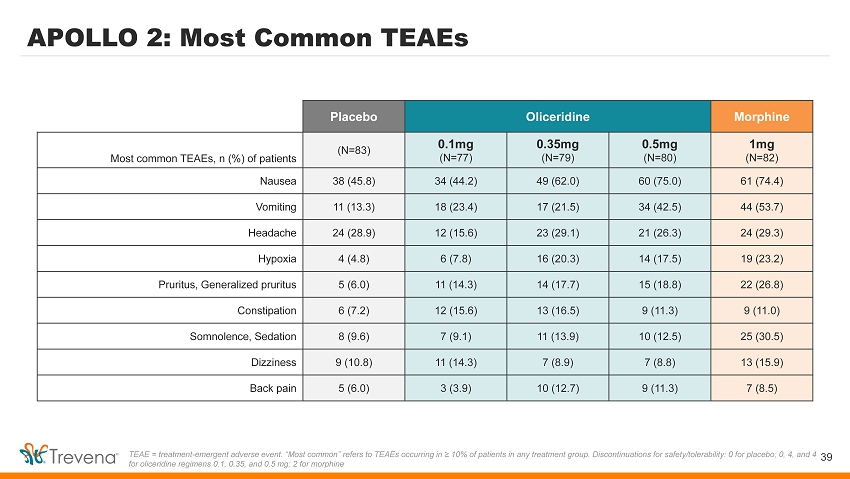
APOLLO 2: Most Common TEAEs 39 TEAE = treatment - emergent adverse event. “Most common” refers to TEAEs occurring in ≥ 10% of patients in any treatment group. Di scontinuations for safety/tolerability: 0 for placebo; 0, 4, and 4 for oliceridine regimens 0.1, 0.35, and 0.5 mg; 2 for morphine Placebo Oliceridine Morphine Most common TEAEs, n (%) of patients (N=83) 0.1mg (N=77) 0.35mg (N=79) 0.5mg (N=80) 1mg (N=82) Nausea 38 (45.8) 34 (44.2) 49 (62.0) 60 (75.0) 61 (74.4) Vomiting 11 (13.3) 18 (23.4) 17 (21.5) 34 (42.5) 44 (53.7) Headache 24 (28.9) 12 (15.6) 23 (29.1) 21 (26.3) 24 (29.3) Hypoxia 4 (4.8) 6 (7.8) 16 (20.3) 14 (17.5) 19 (23.2) Pruritus, Generalized pruritus 5 (6.0) 11 (14.3) 14 (17.7) 15 (18.8) 22 (26.8) Constipation 6 (7.2) 12 (15.6) 13 (16.5) 9 (11.3) 9 (11.0) Somnolence, Sedation 8 (9.6) 7 (9.1) 11 (13.9) 10 (12.5) 25 (30.5) Dizziness 9 (10.8) 11 (14.3) 7 (8.9) 7 (8.8) 13 (15.9) Back pain 5 (6.0) 3 (3.9) 10 (12.7) 9 (11.3) 7 (8.5)
Delta Receptor Agonists Have Unique Benefits Triptans / Ditans • Target: serotonin receptors mediate vascular excitability (a ssociated CV risk) 1 • Migraine - specific treatment CGRPs • Target: CGRP receptors regulate neuronal structures involved in pain signaling 2 • Migraine - specific treatment Delta receptor agonists • Target: delta receptors located in pain pathways; also distributed throughout brain regions associated with sensory information, emotional processing, and reward / impulsivity 3 • Potential for broad therapeutic application 40 Potential utility for a variety of CNS indications 1) Rothrock JF & Friedman DI, American Headache Society website: https://americanheadachesociety.org/wp - content/uploads/2018/05/ John_Rothrock_and_Deborah_Friedman_ - _Triptans.pdf. 2) Durham PL, Headache, 2006. 3) Peppin JF & Raffa RB, Journal of Clinical Pharmacy and Therapeutics, 2015.
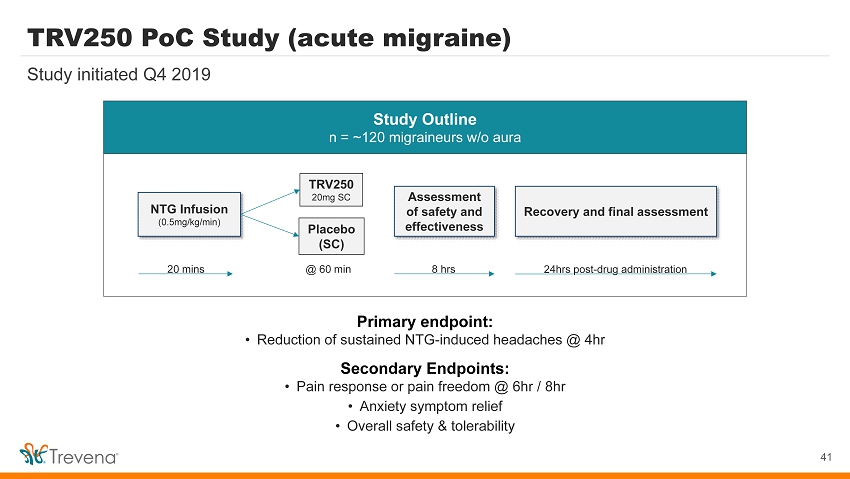
TRV250 PoC Study (acute migraine) 41 Study initiated Q4 2019 Study Outline n = ~120 migraineurs w/o aura Primary endpoint: • Reduction of sustained NTG - induced headaches @ 4hr Secondary Endpoints: • Pain response or pain freedom @ 6hr / 8hr • Anxiety symptom relief • Overall safety & tolerability NTG Infusion (0.5mg/kg/min) 20 mins TRV250 20mg SC Placebo (SC) Assessment of safety and effectiveness @ 60 min 8 hrs Recovery and final assessment 24hrs post - drug administration