EXHIBIT 99.2
Published on May 6, 2021
Exhibit 99.2

INNOVATING FOR PATIENTS Nasdaq TRVN I May 2021
Forward - Looking Statements To the extent that statements contained in this presentation are not descriptions of historical facts regarding Trevena, Inc. (t he “Company” or “we”), they are forward - looking statements reflecting management’s current beliefs and expectations. Forward - looking statements are subject to known and unknown risks, uncertainties, and other factors that may cause our or our industry’s actual results, levels of activity, performance, or achievements to be materially different from those anticipated by such statement s. You can identify forward - looking statements by terminology such as “anticipate,” “believe,” “estimate,” “expect,” “intend,” “may,” “might,” “plan,” “objective,” “predict,” “project,” “suggest, ” “ target,” “potential,” “will,” “would,” “could,” “should,” “continue,” “ongoing,” or the negative of these terms or similar expressions. Forward - looking statements contained in this presentation include, but are n ot limited to, ( i ) statements regarding the timing of anticipated clinical trials for our product candidates; (ii) the timing of receipt of clinical data for our product candidates; (iii) our ex pectations regarding the potential safety, efficacy, or clinical utility of our product candidates; (iv) the size of patient populations targeted by our product candidates and market adoption of our potent ial drugs by physicians and patients; (v) the timing or likelihood of regulatory filings and approvals; and (vi) our cash needs. Actual results may differ materially from those indicated by such forward - looking statements as a result of various important f actors, including: the commercialization of any approved drug product, the status, timing, costs, results and interpretation of our clinical trials or any future trials of any of our inve sti gational drug candidates; the uncertainties inherent in conducting clinical trials; expectations for regulatory interactions, submissions and approvals, including our assessment of the discussions with th e FDA or other regulatory agencies about any and all of our programs; uncertainties related to the commercialization of OLINVYK; available funding; uncertainties related to our intellec tua l property; uncertainties related to the ongoing COVID - 19 pandemic, other matters that could affect the availability or commercial potential of our therapeutic candidates; and other f act ors discussed in the Risk Factors set forth in our Annual Report on Form 10 - K and Quarterly Reports on Form 10 - Q filed with the Securities and Exchange Commission (SEC) and in other filings we mak e with the SEC from time to time. In addition, the forward - looking statements included in this presentation represent our views only as of the date hereof. We anticipate that subsequen t e vents and developments may cause our views to change. However, while we may elect to update these forward - looking statements at some point in the future, we specifically disclaim any obligation to do so, except as may be required by law. 2
BOARD OF DIRECTORS Leon O. Moulder , Jr. Chairman Marvin H. Johnson, Jr. Carrie L. Bourdow Julie H. McHugh Scott Braunstein, M.D. Jake R. Nunn Michael R. Dougherty Anne M. Phillips, M.D. Maxine Gowen, Ph.D. Barbara Yanni SENIOR MANAGEMENT Carrie L. Bourdow President & Chief Executive Officer Scott Applebaum SVP, Chief Legal & Regulatory Officer Mark A. Demitrack, M.D . SVP, Chief Medical Officer Barry Shin SVP, Chief Financial Officer Robert T. Yoder SVP, Chief Commercial Officer Trevena’s Experienced Leadership Team 3

IV OLINVYK: Differentiated profile NCE approved for the management of acute pain in adults Commercial launch in Q1 2021; targeting 100 formulary wins by year - end Large market, targeted launch 45M+ US hospital patients; 9M procedures is initial core focus $1.5B+ market opportunity for core focus Novel CNS pipeline New mechanisms for acute migraine, diabetic neuropathic pain, epilepsy, opioid use disorder NCEs targeting significant unmet needs TRV027 for COVID - 19 Novel MOA to treat COVID - 19 acute lung injury / abnormal clotting Selected for NIH ACTIV and REMAP - CAP trials; up to 600 COVID - 19 patients on TRV027 Strong financial position $97.7M cash and cash equivalents as of 3/31/2021 Funds operations through Q4 2022 Trevena: Innovative CNS Company 4 OLINVYK is indicated in adults for the management of acute pain severe enough to require an intravenous opioid analgesic and for whom alternative treatments are inadequate. Please see Important Safety Information including BOXED WARNING at the end of presentation. Full Prescribing Information at www.OLINVYK.com . NCE = New Chemical Entity; MOA = Mechanism of Action; NIH = National Institutes of Health; ACTIV = Accelerating COVID - 19 Therape utic Interventions and Vaccines; REMAP - CAP = Randomised , Embedded, Multi - factorial, Adaptive Platform Trial for Community - Acquired Pneumonia

PRE - CLINICAL PHASE 1 PHASE 2 PHASE 3 NDA EXPECTED CATALYSTS OLINVYK® New chemical entity (mu - opioid receptor) • Commercial launch ongoing • Cleveland Clinic outcomes study TRV027 Novel AT 1 receptor selective agonist • NIH ACTIV study • REMAP - CAP study TRV250 G - protein selective agonist (delta receptor) • IND - enabling activities (oral) TRV734 G - protein selective agonist (mu - opioid receptor) • PoC study data (NIDA) TRV045 Novel S1P receptor modulator • IND filing • Ph1 initiation Multiple Expected Catalysts 5 Please see Important Safety Information including BOXED WARNING at the end of presentation. Full Prescribing Information at www.OLINVYK.com . TRV250, TRV734, TRV027, and TRV045 are investigational products and are not approved by the FDA or any other regulatory agenc y. ARDS = Acute Respiratory Distress Syndrome; ACTIV = Accelerating COVID - 19 Therapeutic Interventions and Vaccines; REMAP - CAP = Randomised , Embedded, Multi - factorial, Adaptive Platform Trial for Community - Acquired Pneumonia; IND = Investigational New Drug; PoC = Proof - of - Concept Acute pain IV Acute migraine Collaboration with National Institute on Drug Abuse Opioid use disorder oral Diabetic neuropathic pain Epilepsy collaboration with National Institutes of Health ARDS / abnormal clotting (COVID - 19) oral IV Collaborations with NIH ACTIV and REMAP - CAP APPROVED IV oral / SC
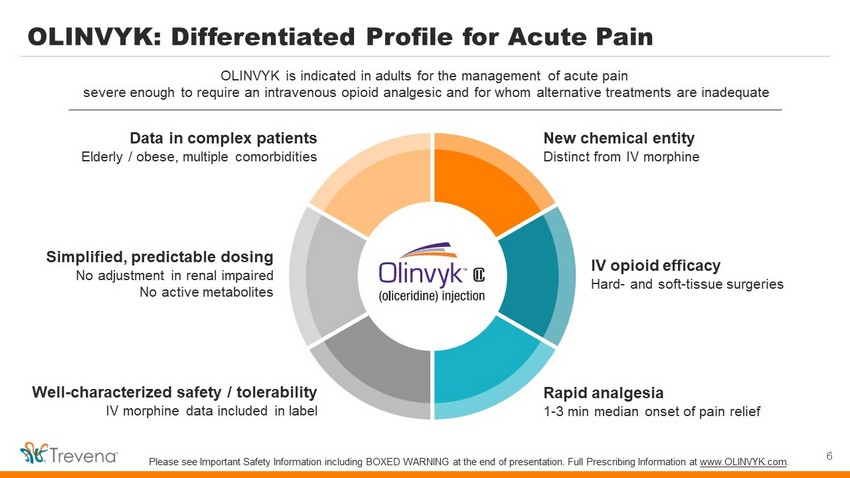
OLINVYK: Differentiated Profile for Acute Pain 6 OLINVYK is indicated in adults for the management of acute pain severe enough to require an intravenous opioid analgesic and for whom alternative treatments are inadequate New chemical entity Distinct from IV morphine IV opioid efficacy Hard - and soft - tissue surgeries Rapid analgesia 1 - 3 min median onset of pain relief Simplified, predictable dosing No adjustment in renal impaired No active metabolites Data in complex patients Elderly / obese, multiple comorbidities Well - characterized safety / tolerability IV morphine data included in label Please see Important Safety Information including BOXED WARNING at the end of presentation. Full Prescribing Information at www.OLINVYK.com .
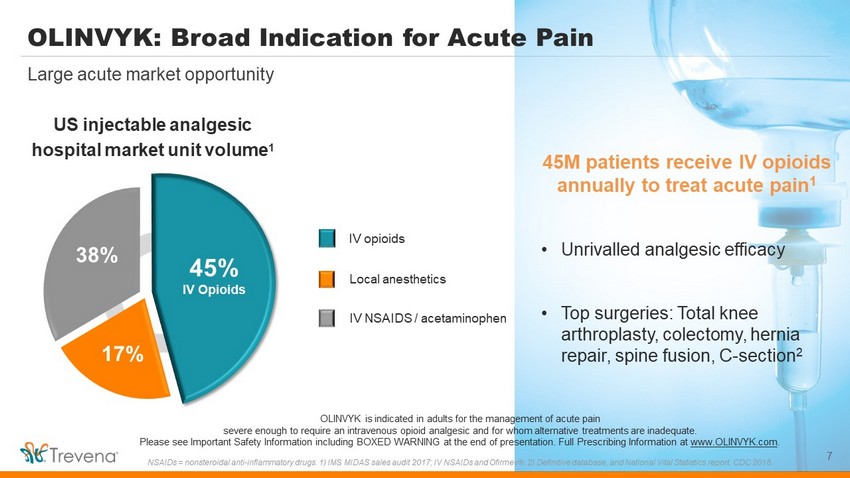
OLINVYK: Broad Indication for Acute Pain 7 Large acute market opportunity 45M patients receive IV opioids annually to treat acute pain 1 • Unrivalled analgesic efficacy • Top surgeries: Total knee arthroplasty, colectomy, hernia repair, spine fusion, C - section 2 IV NSAIDS / acetaminophen US injectable analgesic hospital market unit volume 1 IV opioids 45% IV Opioids 17% 38% Local anesthetics OLINVYK is indicated in adults for the management of acute pain severe enough to require an intravenous opioid analgesic and for whom alternative treatments are inadequate. Please see Important Safety Information including BOXED WARNING at the end of presentation. Full Prescribing Information at www.OLINVYK.com . NSAIDs = nonsteroidal anti - inflammatory drugs. 1) IMS MIDAS sales audit 2017; IV NSAIDs and Ofirmev ®. 2) Definitive database, and National Vital Statistics report, CDC 2018.
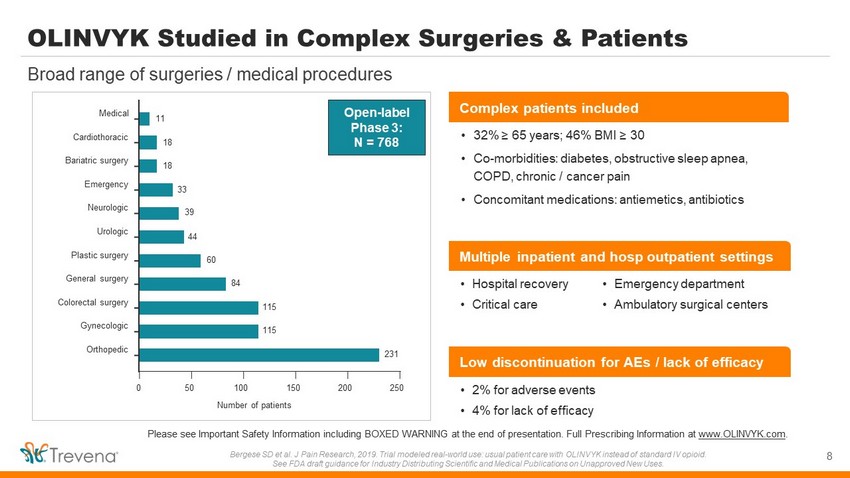
8 Broad range of surgeries / medical procedures Please see Important Safety Information including BOXED WARNING at the end of presentation. Full Prescribing Information at www.OLINVYK.com . Bergese SD et al. J Pain Research, 2019. Trial modeled real - world use: usual patient care with OLINVYK instead of standard IV opioid. See FDA draft guidance for Industry Distributing Scientific and Medical Publications on Unapproved New Uses. 0 50 100 150 200 250 Orthopedic Gynecologic Colorectal surgery General surgery Plastic surgery Urologic Neurologic Emergency Bariatric surgery Cardiothoracic Medical Number of patients 11 18 18 33 39 44 60 84 115 115 231 Open - label Phase 3: N = 768 • 2% for adverse events • 4% for lack of efficacy • Hospital recovery • Critical care • Emergency department • Ambulatory surgical centers • 32% ≥ 65 years; 46% BMI ≥ 30 • Co - morbidities: diabetes, obstructive sleep apnea, COPD, chronic / cancer pain • Concomitant medications: antiemetics, antibiotics Multiple inpatient and hosp outpatient settings Complex patients included Low discontinuation for AEs / lack of efficacy OLINVYK Studied in Complex Surgeries & Patients
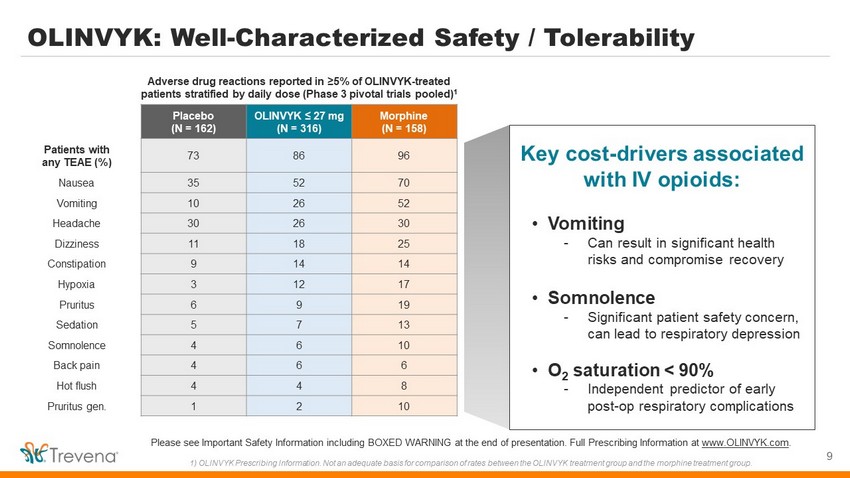
OLINVYK: Well - Characterized Safety / Tolerability 9 Please see Important Safety Information including BOXED WARNING at the end of presentation. Full Prescribing Information at www.OLINVYK.com . 1) OLINVYK Prescribing Information. N ot an adequate basis for comparison of rates between the OLINVYK treatment group and the morphine treatment group. Placebo (N = 162) OLINVYK ≤ 27 mg (N = 316) Morphine (N = 158) Patients with any TEAE (%) 73 86 96 Nausea 35 52 70 Vomiting 10 26 52 Headache 30 26 30 Dizziness 11 18 25 Constipation 9 14 14 Hypoxia 3 12 17 Pruritus 6 9 19 Sedation 5 7 13 Somnolence 4 6 10 Back pain 4 6 6 Hot flush 4 4 8 Pruritus gen. 1 2 10 Adverse drug reactions reported in ≥5% of OLINVYK - treated patients stratified by daily dose (Phase 3 pivotal trials pooled) 1 Key cost - drivers associated with IV opioids: • Vomiting - Can result in significant health risks and compromise recovery • Somnolence - Significant patient safety concern, can lead to respiratory depression • O 2 saturation < 90% - Independent predictor of early post - op respiratory complications
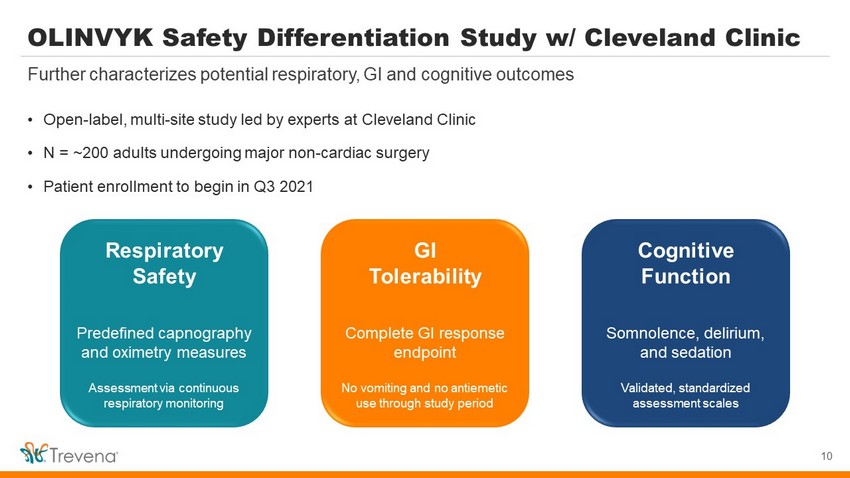
OLINVYK Safety Differentiation Study w/ Cleveland Clinic • Open - label, multi - site study led by experts at Cleveland Clinic • N = ~200 adults undergoing major non - cardiac surgery • Patient enrollment to begin in Q3 2021 10 Further characterizes potential respiratory, GI and cognitive outcomes Respiratory Safety Predefined c apnography and oximetry measures Assessment via continuous respiratory monitoring GI Tolerability Complete GI response endpoint No vomiting and no antiemetic use through study period Cognitive Function Somnolence, delirium, and sedation Validated, standardized assessment scales

OLINVYK: Ease of Dosing and Administration • Bolus Dosing: 1 mg and 2 mg vials (single dose) • PCA Dosing: 30 mg vial (single patient use) • OLINVYK 1 mg ≈ morphine 5 mg 1 27 mg cumulative daily dose limit Do not administer single doses greater than 3 mg 11 3 vials allow for flexible and tailored IV dosing Please see Important Safety Information including BOXED WARNING at the end of presentation. Full Prescribing Information at www.OLINVYK.com . 1) For an initial dose. PCA = Patient - Controlled Analgesia No refrigeration / reconstitution For PCA use only $17.50 $25.75 $110.00 WAC: 1 mg / 1mL 30 mg / 30 mL 2 mg / 2mL ~$100 / day (estimated avg cost across procedures)
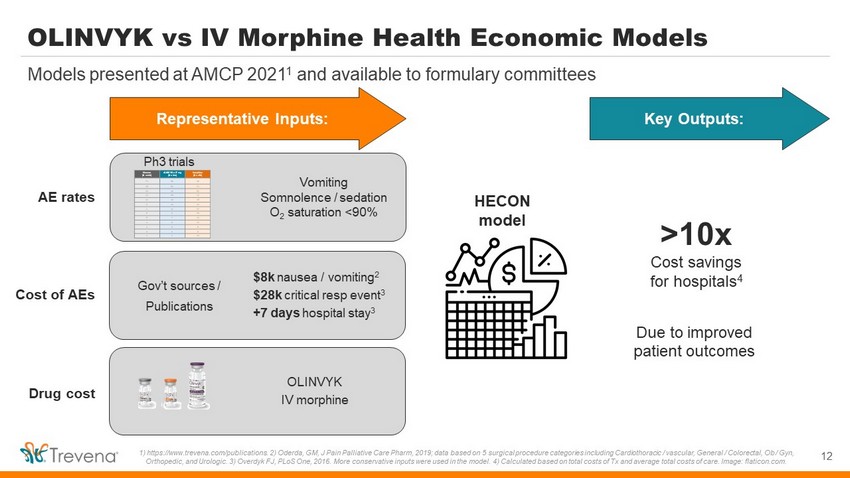
OLINVYK vs IV Morphine Health Economic Models 12 Models presented at AMCP 2021 1 and available to formulary committees 1) https://www.trevena.com/publications. 2) Oderda , GM, J Pain Palliative Care Pharm, 2019; data based on 5 surgical procedure categories including Cardiothoracic / vascular, Gen eral / Colorectal, Ob / Gyn, Orthopedic, and Urologic. 3) Overdyk FJ, PLoS One, 2016. More conservative inputs were used in the model. 4) Calculated based on total costs of Tx and average total costs of care. Image: flaticon.com. Vomiting Somnolence / sedation O 2 saturation <90% Representative Inputs: >10x Cost savings for hospitals 4 Due to improved patient outcomes HECON model Placebo (N = 162) OLINVYK ≤ 27 mg (N = 316) Morphine (N = 158) Patients with any TEAE (%) 73 86 96 Nausea 35 52 70 Vomiting 10 26 52 Headache 30 26 30 Dizziness 11 18 25 Constipation 9 14 14 Hypoxia 3 12 17 Pruritus 6 9 19 Sedation 5 7 13 Somnolence 4 6 10 Back pain 4 6 6 Hot flush 4 4 8 Pruritus gen. 1 2 10 AE rates Cost of AEs Drug cost Ph3 trials Gov’t sources / Publications $8k nausea / vomiting 2 $28k critical resp event 3 +7 days hospital stay 3 OLINVYK IV morphine Key Outputs:

Customer Engagement Strategy 13

Targeted Account Launch as of Q1 2021 ~40 account reps / MSLs deployed Q1 2021 • OLINVYK: NCE, distinct from IV morphine • 1 - 3 min onset & no active metabolites • Safety data in complex patients / surgeries • OLINVYK published safety data vs. IV morphine • Published health economic / cost offset data* Health Care Practitioners (HCPs) Please see Important Safety Information including BOXED WARNING at the end of presentation. Full Prescribing Information at www.OLINVYK.com . MSL = Medical Science Liaison; NCE = New Chemical Entity. Images: flaticon.com. Hospitals ASCs Targeted Accounts Anesthesiology, Orthopedic, Colorectal, Gynecologic 550 hospitals and 500 ambulatory surgery centers
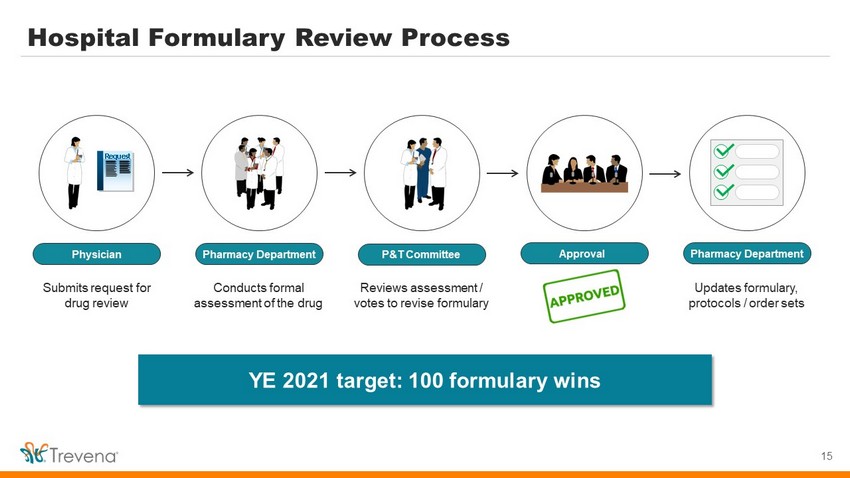
Hospital Formulary Review Process 15 Physician Pharmacy Department P&T Committee Approval Pharmacy Department Submits request for drug review C onducts formal assessment of the drug R eviews assessment / votes to revise formulary Updates formulary, protocols / order sets Request YE 2021 target: 100 formulary wins
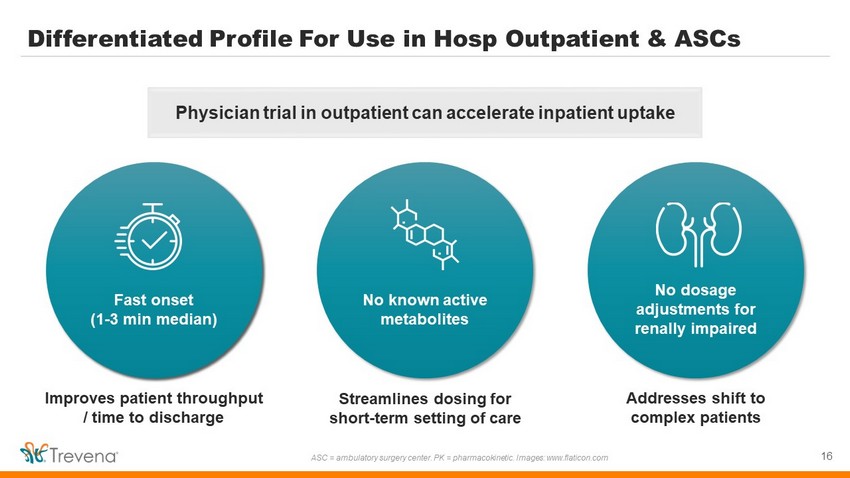
Differentiated Profile For Use in Hosp Outpatient & ASCs 16 ASC = ambulatory surgery center. PK = pharmacokinetic. Images: www.flaticon.com Fast onset (1 - 3 min median) No known active metabolites No dosage adjustments for renally impaired Improves patient throughput / time to discharge Streamlines dosing for short - term setting of care Addresses shift to complex patients Physician trial in outpatient can accelerate inpatient uptake

OLINVYK: Significant Opportunity in Acute Pain 17 Please see Important Safety Information including BOXED WARNING at the end of presentation. Full Prescribing Information at www.OLINVYK.com . Source: Definitive Healthcare; American Hospital Association. *Assumes ~$100 / day price for oliceridine 2032 composition of matter patent expiration does not include potential patent extensions. Specialty Targets Patient & Procedure Risk Initial launch focus ~45 M patients Initial core focus (9 M ) Expanded areas of focus (28 M ) • Hospitals / ambulatory surgical centers • “CORES” patient focus: comorbid, obese, renal, elderly, sleep apnea Initial core focus (9 M ) ~15 M days of therapy (initial focus) = $1.5B+ market opportunity* • Leverage respiratory and GI safety vs. IV morphine to expand surgical procedures • Cognitive function & additional HECON Expanded areas of focus (28 M ) 2032+ COM Patent
We Continue to Learn from and Adapt to COVID - 19 Challenges • No delays in regulatory timelines; approval and DEA scheduling in 2H 2020 • Commercial supply of all 3 presentations made available to customers Transitioned into commercial organization with minimal business interruption • Procedure volumes may be slow to recover; backlog of elective surgeries building 1 • IV drug shortages, increase in patient acuity continue to pressure healthcare systems What we learned from our customers • COVID - 19 will continue impacting our customers; OLINVYK’s value proposition remains relevant • We will be making informed resource deployment decisions throughout first year of launch Considerations for a successful field launch in 2021 18 1) Kaufman Hall 2020 State of Healthcare Performance Improvement Report: The Impact of COVID - 19, October 2020.

TRV027 NCE targeting the AT 1 receptor in COVID - 19 19
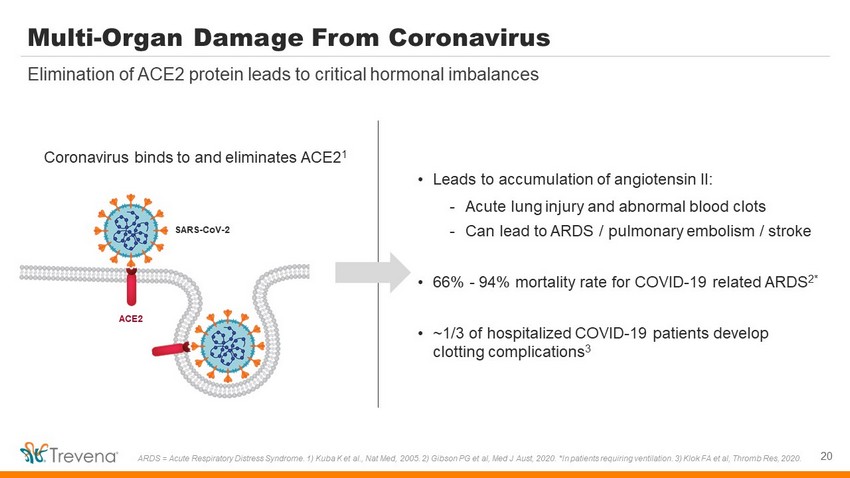
Multi - Organ Damage From Coronavirus 20 Elimination of ACE2 protein leads to critical hormonal imbalances ARDS = Acute Respiratory Distress Syndrome. 1) Kuba K et al., Nat Med, 2005. 2) Gibson PG et al, Med J Aust, 2020. *In patients requiring ventilation. 3) Klok FA et al, Thromb Res, 2020. SARS - CoV - 2 ACE2 Coronavirus binds to and eliminates ACE2 1 • Leads to accumulation of angiotensin II: - Acute lung injury and abnormal blood clots - Can lead to ARDS / pulmonary embolism / stroke • 66% - 94% mortality rate for COVID - 19 related ARDS 2* • ~1/3 of hospitalized COVID - 19 patients develop clotting complications 3
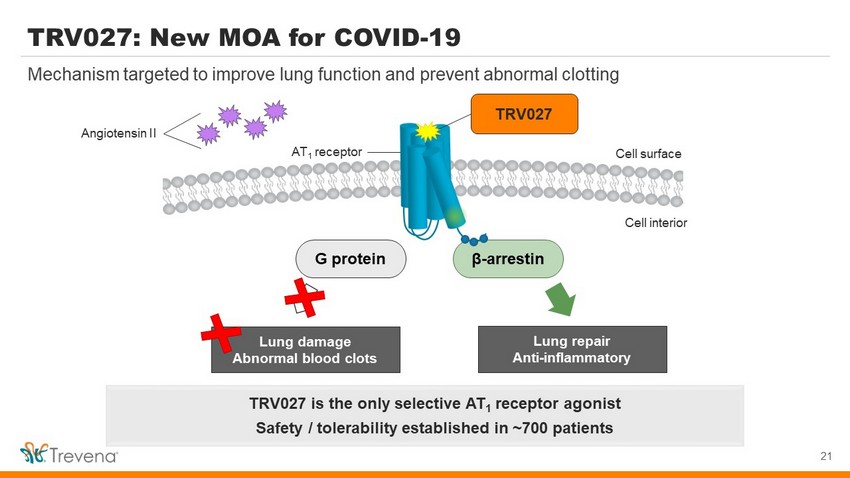
TRV027 β - arrestin TRV027: New MOA for COVID - 19 21 Mechanism targeted to improve lung function and prevent abnormal clotting AT 1 receptor TRV027 is the only selective AT 1 receptor agonist Safety / tolerability established in ~700 patients G protein Cell surface Cell interior Lung damage Abnormal blood c lots Lung repair Anti - inflammatory Angiotensin II

TRV027 COVID - 19 Study - Vanderbilt UMC (ACTIV - 4d) • Part of NIH’s ongoing ACTIV* public - private partnership • Multi - site, multi - arm, placebo - controlled trial • ~300 COVID - 19 patients ≥18 years old treated with TRV027 22 NIH - funded trial with Vanderbilt University Medical Center as lead coordinating site Key outcomes to be studied: Recovery Supplemental O 2 use Mechanical ventilation Mortality *ACTIV = Accelerating COVID - 19 Therapeutic Interventions and Vaccines
TRV027 COVID - 19 Study - REMAP - CAP • Multi - site, adaptive, Phase 2 / 3 trial in hospitalized COVID - 19 patients (≥18 years)* • 200 - 300 COVID - 19 patients treated with TRV027 • TRV027 administered (open label) in conjunction w/ACE inhibitor 23 Funded by REMAP - CAP, a global clinical trial network led by experts in pandemic response Primary outcome: In - hospital mortality + Organ failure support in ICU (21 days post - randomization) Additional outcomes: ICU / hospital length of stay, ventilator - free days, organ failure - free days * Includes patients admitted to ICU
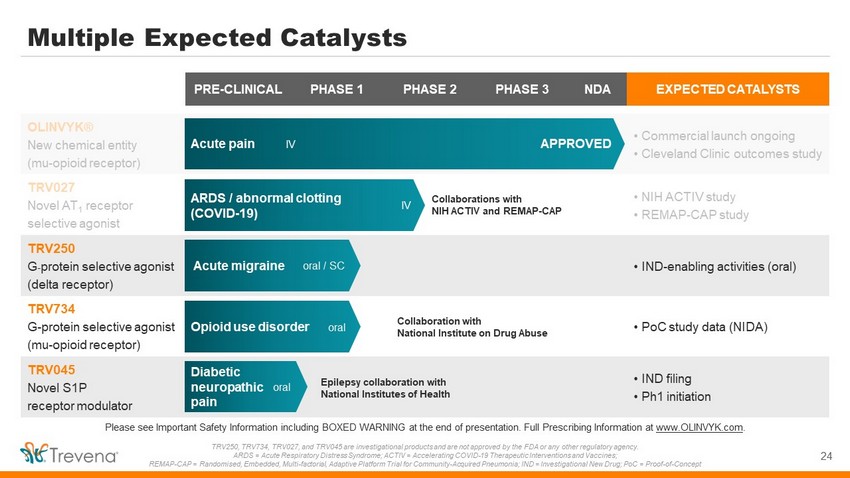
PRE - CLINICAL PHASE 1 PHASE 2 PHASE 3 NDA EXPECTED CATALYSTS OLINVYK® New chemical entity (mu - opioid receptor) • Commercial launch ongoing • Cleveland Clinic outcomes study TRV027 Novel AT 1 receptor selective agonist • NIH ACTIV study • REMAP - CAP study TRV250 G - protein selective agonist (delta receptor) • IND - enabling activities (oral) TRV734 G - protein selective agonist (mu - opioid receptor) • PoC study data (NIDA) TRV045 Novel S1P receptor modulator • IND filing • Ph1 initiation Multiple Expected Catalysts 24 Please see Important Safety Information including BOXED WARNING at the end of presentation. Full Prescribing Information at www.OLINVYK.com . TRV250, TRV734, TRV027, and TRV045 are investigational products and are not approved by the FDA or any other regulatory agenc y. ARDS = Acute Respiratory Distress Syndrome; ACTIV = Accelerating COVID - 19 Therapeutic Interventions and Vaccines; REMAP - CAP = Randomised , Embedded, Multi - factorial, Adaptive Platform Trial for Community - Acquired Pneumonia; IND = Investigational New Drug; PoC = Proof - of - Concept Acute pain IV Acute migraine Collaboration with National Institute on Drug Abuse Opioid use disorder oral Diabetic neuropathic pain Epilepsy collaboration with National Institutes of Health ARDS / abnormal clotting (COVID - 19) oral IV Collaborations with NIH ACTIV and REMAP - CAP APPROVED IV oral / SC

TRV250: New MOA for Acute Treatment of Migraine 25 Delta receptor: Untapped potential in CNS space Migraine represents a large market opportunity; total migraine drug market = ~$3.5B 1) Data from Decision Resources, Pharmacor migraine market landscape and forecast 2018. 2) Moven et al., J Neurol Neurosurg Psychiatry, 2016. Icons made by Freepik from www.flaticon.com Play important role in regulation of pain, mood, and anxiety Delta receptors have unique distribution throughout the brain 650M migraines treated each year 1.2M ER visits due to migraines • 20 - 30% of migraine sufferers do not respond to / cannot tolerate the market - leading triptan drug class • Approx. 50% of migraineurs also suffer from anxiety 2 Every year in the US 1 :

TRV250: Well - Tolerated in Ph1 Healthy Volunteer PK Study • Well tolerated, with no SAEs across broad range of doses • Predictable PK: dose - proportional between 0.1 mg to 30 mg SC • Half - life consistent across all doses • No EEG findings observed in any subject Subcutaneous doses up to 30 mg studied; no SAEs observed SC = subcutaneous. Fossler MJ et al., CNS Drugs, Aug 2020;34(8):853 - 865. Single dose pharmacokinetics of TRV250 given by SC injection IND - enabling activities initiated for new oral dose form
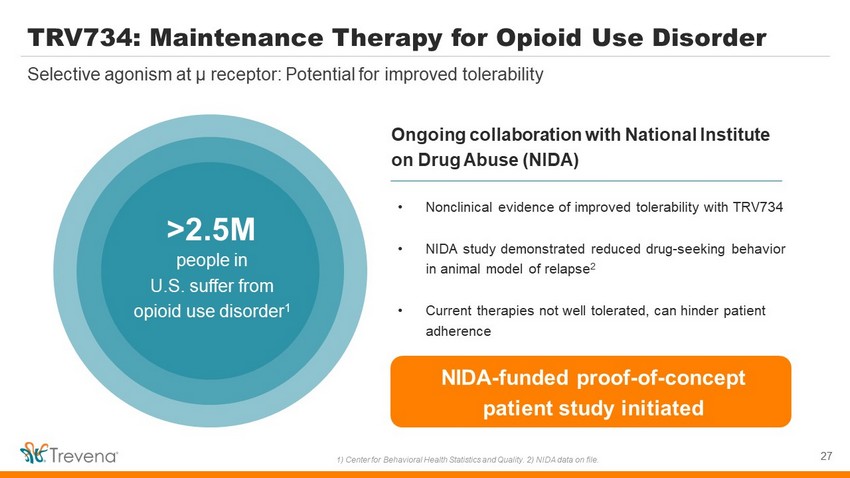
TRV734: Maintenance Therapy for Opioid Use Disorder 27 Selective agonism at µ receptor: Potential for improved tolerability 1) Center for Behavioral Health Statistics and Quality. 2) NIDA data on file. Ongoing collaboration with National Institute on Drug Abuse (NIDA) >2.5M people in U.S. suffer from opioid use disorder 1 • Nonclinical evidence of improved tolerability with TRV734 • NIDA study demonstrated reduced drug - seeking behavior in animal model of relapse 2 • Current therapies not well tolerated, can hinder patient adherence NIDA - funded proof - of - concept patient study initiated
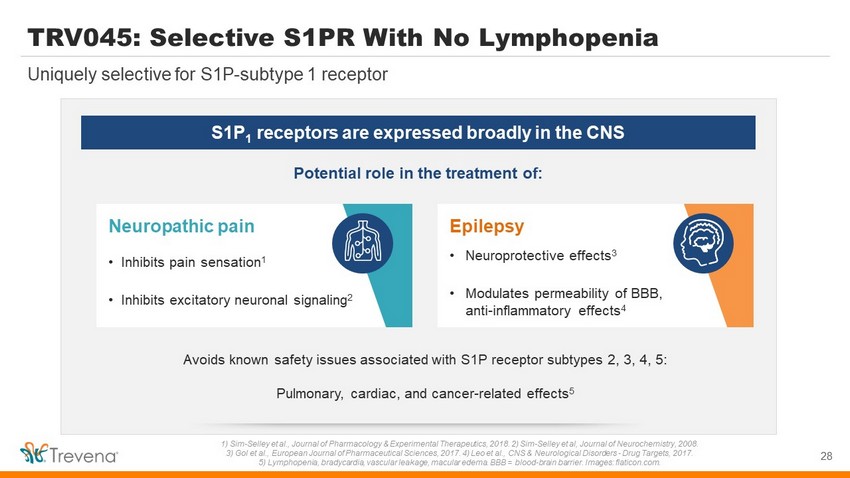
TRV045: Selective S1PR With No Lymphopenia 28 Uniquely selective for S1P - subtype 1 receptor 1) Sim - Selley et al., Journal of Pharmacology & Experimental Therapeutics, 2018. 2) Sim - Selley et al, Journal of Neurochemistry, 2008. 3) Gol et al., European Journal of Pharmaceutical Sciences, 2017. 4) Leo et al., CNS & Neurological Disorders - Drug Targets, 20 17. 5) Lymphopenia, bradycardia, vascular leakage, macular edema. BBB = blood - brain barrier. Images: flaticon.com. S1P 1 receptors are expressed broadly in the CNS Potential role in the treatment of: Neuropathic pain • Inhibits pain sensation 1 • Inhibits excitatory neuronal signaling 2 Avoids known safety issues associated with S1P receptor subtypes 2, 3, 4, 5: Pulmonary, cardiac, and cancer - related effects 5 Epilepsy • Neuroprotective effects 3 • Modulates permeability of BBB, anti - inflammatory effects 4

Avoids Lymphopenia Reverses Pain Response TRV045: Novel MOA for Diabetic Neuropathic Pain 0 20 40 60 80 100 Fingolimod TRV045 29 1) Rosenberger et al., Journal of Neural Transmission, 2020 and CDC National Diabetes Statistics Report, 2020. 2) Shillo et al., Current Diabetes Reports, 2019. 3) American Diabetes Association. 4) FDA product labels for Lyrica, Lyrica CR, Cymbalta, Nucynta ER, and Qutenza , Tesfaye et.al. Pain (2013). 5) Sadosky et. al., J Diabetes Complications 2015. 6) CIPN mouse model: Paclitaxel 6 mg/kg, i.p. on Days 1, 3, 5, 7. Hyperalgesia measured as % non - response to 0.4 g Von Frey filament vs. baseline, tested 30’ after dosing on Day 13. Lymphocytes measured after 3 days of dosing. Data are mean s.e.m. n=5 - 7 mice/group. *p<0.05 or **p<0.01 vs. control • DNP affects ~25% of people w/ diabetes 2 - Approved agents inadequate for ~50% of patients 3,4 - ~4x direct costs for DNP patients (vs diabetes alone) 5 • In animals, TRV045 reversed neuropathic pain without immune - suppressing activity 6 • Non - opioid MOA with broad potential for CNS indications - IND filing for DNP in 1H 2021 - Epilepsy evaluation (NIH) ongoing 0 1 2 3 4 5 6 Fingolimod TRV045 peripheral lymphocytes (10 3 cells / m L) % non - response to pain stimulus 0.03 mg/kg po 1.0 mg/kg sc 0.03 mg/kg po 3.7 mg/kg sc Paclitaxel - induced hyperalgesia Vehicle alone No reduction despite 3.7x dosing (vs. above) ** * ** 5M+ people (US) suffer from DNP, with limited therapeutic options 1

IV OLINVYK: Differentiated profile NCE approved for the management of acute pain in adults Commercial launch in Q1 2021; targeting 100 formulary wins by year - end Large market, targeted launch 45M+ US hospital patients; 9M procedures is initial core focus $1.5B+ market opportunity for core focus Novel CNS pipeline New mechanisms for acute migraine, diabetic neuropathic pain, epilepsy, opioid use disorder NCEs targeting significant unmet needs TRV027 for COVID - 19 Novel MOA to treat COVID - 19 acute lung injury / abnormal clotting Selected for NIH ACTIV and REMAP - CAP trials; up to 600 COVID - 19 patients on TRV027 Strong financial position $97.7M cash and cash equivalents as of 3/31/2021 Funds operations through Q4 2022 Trevena: Innovative CNS Company 30 OLINVYK is indicated in adults for the management of acute pain severe enough to require an intravenous opioid analgesic and for whom alternative treatments are inadequate. Please see Important Safety Information including BOXED WARNING at the end of presentation. Full Prescribing Information at www.OLINVYK.com . NCE = New Chemical Entity; MOA = Mechanism of Action; NIH = National Institutes of Health; ACTIV = Accelerating COVID - 19 Therape utic Interventions and Vaccines; REMAP - CAP = Randomised , Embedded, Multi - factorial, Adaptive Platform Trial for Community - Acquired Pneumonia

APPENDIX 31
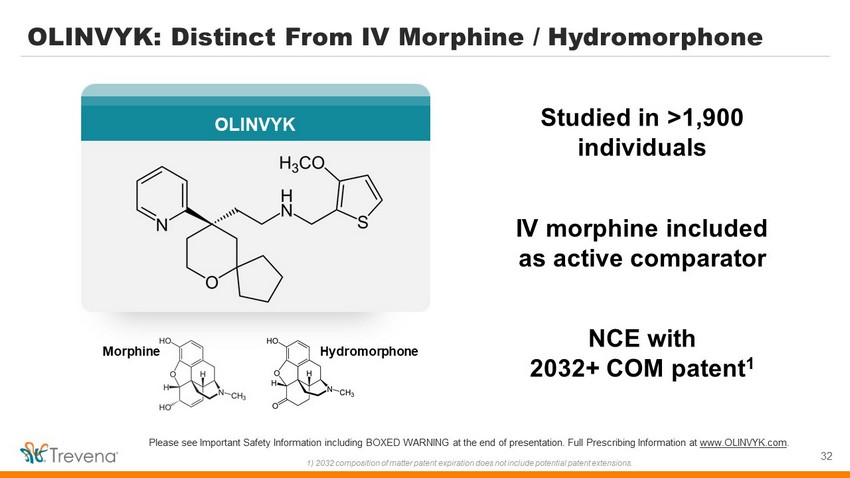
Studied in >1,900 individuals IV morphine included as active comparator NCE with 2032+ COM patent 1 Hydromorphone OLINVYK: Distinct From IV Morphine / Hydromorphone Morphine 32 OLINVYK Please see Important Safety Information including BOXED WARNING at the end of presentation. Full Prescribing Information at www.OLINVYK.com . 1) 2032 composition of matter patent expiration does not include potential patent extensions.
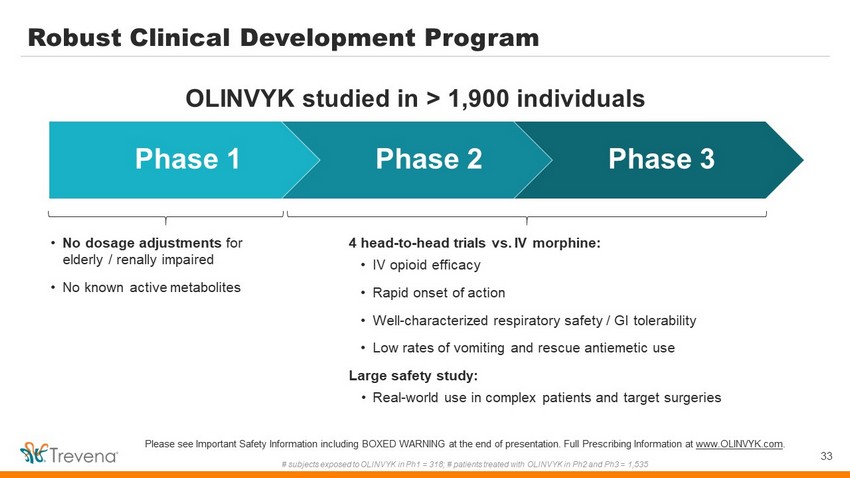
• No dosage adjustments for elderly / renally impaired • No known active metabolites Robust Clinical Development Program 33 Please see Important Safety Information including BOXED WARNING at the end of presentation. Full Prescribing Information at www.OLINVYK.com . # subjects exposed to OLINVYK in Ph1 = 318; # patients treated with OLINVYK in Ph2 and Ph3 = 1,535 Phase 1 Phase 2 Phase 3 4 head - to - head trials vs. IV morphine: • IV opioid efficacy • Rapid onset of action • Well - characterized respiratory safety / GI tolerability • Low rates of vomiting and rescue antiemetic use Large safety study: • Real - world use in complex patients and target surgeries OLINVYK studied in > 1,900 individuals

Superior pain relief vs. placebo (p<0.02) Soft Tissue (SPID - 24) OLINVYK: IV Opioid Efficacy and Rapid Onset 34 • Efficacy achieved in hard tissue & soft tissue models • Rapid onset: perceptible pain relief within 2 - 5 minutes • OLINVYK efficacy data in peer - reviewed journals The Journal of Pain Research 1 and Pain Practice 2 Rapid onset (2 - 5 min) & ~3 hour duration Superior pain relief vs. placebo (p<0.01) Hard Tissue (SPID - 48) Please see Important Safety Information including BOXED WARNING at the end of presentation. Full Prescribing Information at www.OLINVYK.com . 1) Viscusi ER et al. J Pain Res. 2019;12:927 – 943. Published 2019 Mar 11. 2) Singla NK et al. Pain Pract. 2019;19:715 - 731. Publis hed 2019 Jun 04.
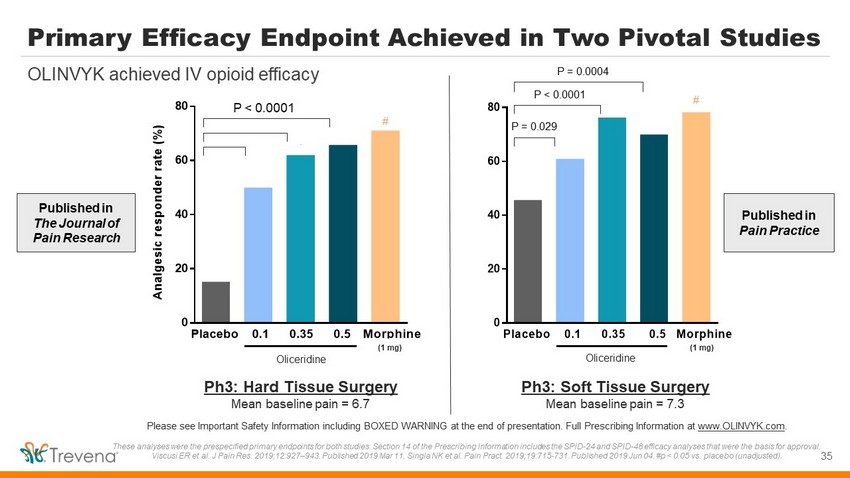
35 Please see Important Safety Information including BOXED WARNING at the end of presentation. Full Prescribing Information at www.OLINVYK.com . These analyses were the prespecified primary endpoints for both studies. Section 14 of the Prescribing Information includes t he SPID - 24 and SPID - 48 efficacy analyses that were the basis for approval. Viscusi ER et al. J Pain Res. 2019;12:927 – 943. Published 2019 Mar 11. Singla NK et al. Pain Pract . 2019;19:715 - 731. Published 2019 Jun 04. #p < 0.05 vs. placebo (unadjusted). 0 20 40 60 80 Placebo 0.1 0.35 0.5 Morphine *** Olinvo Regimen * ** # P = 0.029 P < 0.0001 P = 0.0004 Oliceridine Ph3: Soft Tissue Surgery Mean baseline pain = 7.3 (1 mg) Published in The Journal of Pain Research Published in Pain Practice 0 20 40 60 80 Placebo 0.1 0.35 0.5 Morphine * A n a l g e s i c r e s p o n d e r r a t e ( % ) Olinvo Regimen * * Ph3: Hard Tissue Surgery Mean baseline pain = 6.7 # P < 0.0001 Oliceridine (1 mg) Primary Efficacy Endpoint Achieved in Two Pivotal Studies OLINVYK achieved IV opioid efficacy
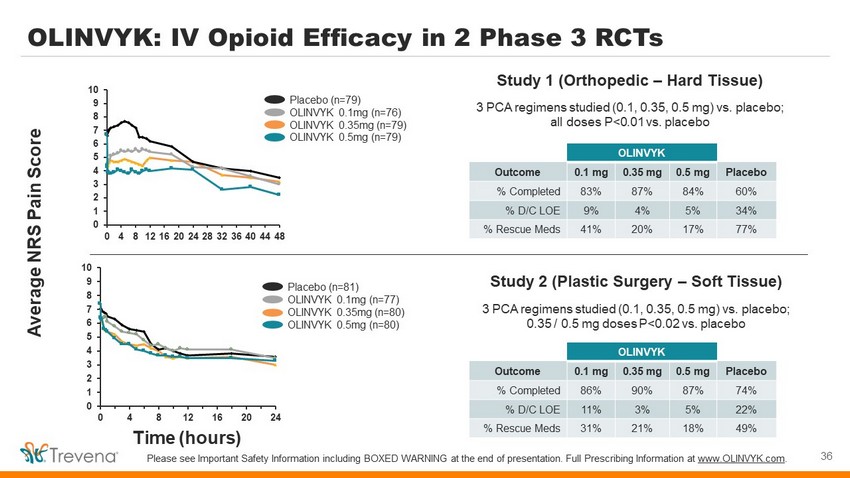
0 1 2 3 4 5 6 7 8 9 10 0 4 8 12 16 20 24 28 32 36 40 44 48 0 1 2 3 4 5 6 7 8 9 10 0 4 8 12 16 20 24 Time (hours) Average NRS Pain Score OLINVYK: IV Opioid Efficacy in 2 Phase 3 RCTs Study 1 (Orthopedic – Hard Tissue) 3 PCA regimens studied (0.1, 0.35, 0.5 mg) vs. placebo; all doses P<0.01 vs. placebo 36 Please see Important Safety Information including BOXED WARNING at the end of presentation. Full Prescribing Information at www.OLINVYK.com . OLINVYK Outcome 0.1 mg 0.35 mg 0.5 mg Placebo % Completed 83% 87% 84% 60% % D/C LOE 9% 4% 5% 34% % Rescue Meds 41% 20% 17% 77% Study 2 (Plastic Surgery – Soft Tissue) 3 PCA regimens studied (0.1, 0.35, 0.5 mg) vs. placebo; 0.35 / 0.5 mg doses P<0.02 vs. placebo OLINVYK Outcome 0.1 mg 0.35 mg 0.5 mg Placebo % Completed 86% 90% 87% 74% % D/C LOE 11% 3% 5% 22% % Rescue Meds 31% 21% 18% 49% Placebo (n=79) OLINVYK 0.1mg (n=76) OLINVYK 0.35mg (n=79) OLINVYK 0.5mg (n=79) Placebo (n=81) OLINVYK 0.1mg (n=77) OLINVYK 0.35mg (n=80) OLINVYK 0.5mg (n=80)

Robust Assessment of Respiratory Safety in Phase 3 RCTs 37 Data included in AMCP dossier used in formulary review 1) Figure 2 - 8, Section 2.2, OLINVYK Evidence Dossier for Formulary Consideration. 2) Figures 3 - 4 and 3 - 8, Section 3.1, OLINVYK E vidence Dossier for Formulary Consideration. • Prespecified secondary endpoint: Respiratory Safety Burden (RSB) - Calculated based on incidence and cumulative duration of respiratory safety events • Full characterization of respiratory safety profile has been made available to HCPs and formulary decision makers - Data can be found in OLINVYK AMCP dossier and published literature Ph3 Respiratory Safety Events 2 (Components of the RSB calculation) Hard Tissue Soft Tissue bpm = breaths per minute; MRPSS = Moline - Roberts Pharmacologic Sedation Scale Ph3 Respiratory Safety Burden 1 Hard Tissue Soft Tissue
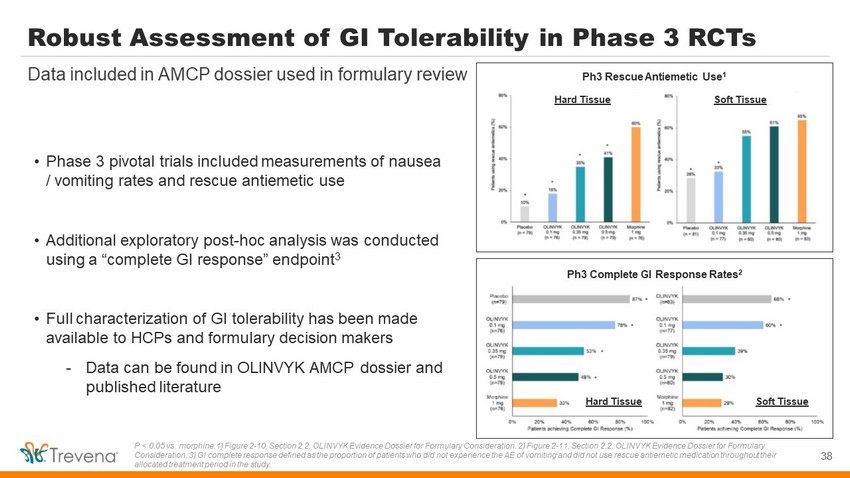
Robust Assessment of GI Tolerability in Phase 3 RCTs 38 Data included in AMCP dossier used in formulary review P < 0.05 vs. morphine.1) Figure 2 - 10, Section 2.2, OLINVYK Evidence Dossier for Formulary Consideration. 2) Figure 2 - 11, Section 2.2, OLINVYK Evidence Dossier for Formulary Consideration. 3) GI complete response defined as the proportion of patients who did not experience the AE of vomiting and di d n ot use rescue antiemetic medication throughout their allocated treatment period in the study. Ph3 Rescue Antiemetic Use 1 Hard Tissue Soft Tissue Ph3 Complete GI Response Rates 2 Hard Tissue Soft Tissue • Phase 3 pivotal trials included measurements of nausea / vomiting rates and rescue antiemetic use • Additional exploratory post - hoc analysis was conducted using a “complete GI response” endpoint 3 • Full characterization of GI tolerability has been made available to HCPs and formulary decision makers - Data can be found in OLINVYK AMCP dossier and published literature

Customer Facing Organization • Allows for execution speed and flexibility in deployment • Full range support: source, hire, train and deploy customer - facing roles • Ability to flex as business needs evolve 39 Partnering with Syneos Health to provide “best in class” commercial support • Sales : Institutional Account Managers • Trade & Access : Regional Account Managers • Medical : Medical Science Liaisons 40 Customer - Facing Roles
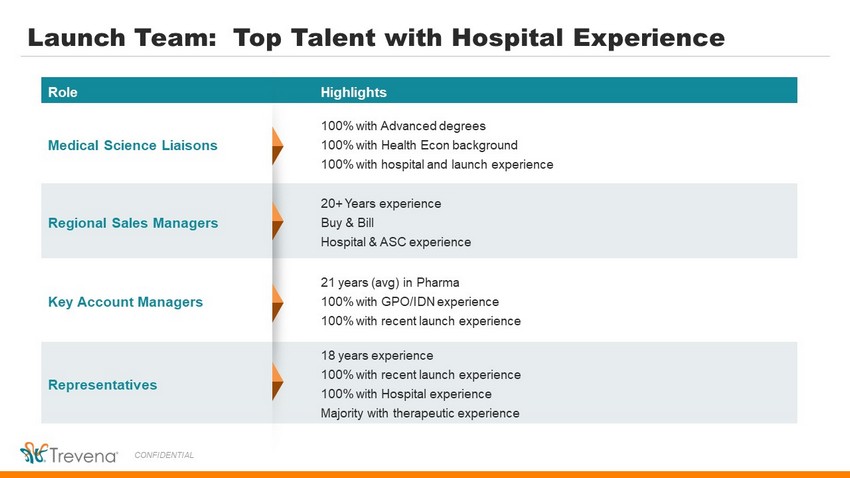
Launch Team: Top Talent with Hospital Experience CONFIDENTIAL Role Highlights Medical Science Liaisons 100% with Advanced degrees 100% with Health Econ background 100% with hospital and launch experience Regional Sales Managers 20+ Years experience Buy & Bill Hospital & ASC experience Key Account Managers 21 years (avg) in Pharma 100% with GPO/IDN experience 100% with recent launch experience Representatives 18 years experience 100% with recent launch experience 100% with Hospital experience Majority with therapeutic experience
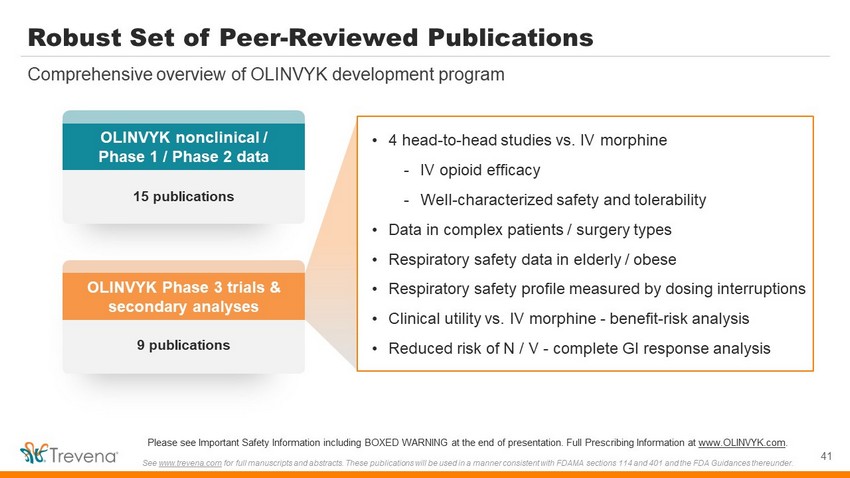
Robust Set of Peer - Reviewed Publications 41 Comprehensive overview of OLINVYK development program • 4 head - to - head studies vs. IV morphine - IV opioid efficacy - Well - characterized safety and tolerability • Data in complex patients / surgery types • Respiratory safety data in elderly / obese • Respiratory safety profile measured by dosing interruptions • Clinical utility vs. IV morphine - benefit - risk analysis • Reduced risk of N / V - complete GI response analysis OLINVYK nonclinical / Phase 1 / Phase 2 data 15 publications OLINVYK Phase 3 trials & secondary analyses 9 publications Please see Important Safety Information including BOXED WARNING at the end of presentation. Full Prescribing Information at www.OLINVYK.com . See www.trevena.com for full manuscripts and abstracts. These publications will be used in a manner consistent with FDAMA sections 114 and 401 an d the FDA Guidances thereunder.

Positive Feedback from Formulary Stakeholders 1 42 Please see Important Safety Information including BOXED WARNING at the end of presentation. Full Prescribing Information at www.OLINVYK.com . 1) Qualitative Pricing research, Charles River Associates, April 2020. 2) “Are the improvements in respiratory safety events and GI tolerability clinically meaningful?” Based on OLINVYK Ph3 clinical trial data. ~75% of formulary stakeholders find OLINVYK’s published data clinically meaningful: 2 66 41 23 14 13 2 0 20 40 60 80 IV morphine IV hydromorphone IV fentanyl Ofirmev Exparel Other Number of Mentions Likely to Replace in Practice (n=100; multiple responses permitted) Key Endpoint (vs. IV morphine) Pharmacist (n=50) Physician (n=50) Respiratory Safety Events and GI Tolerability 72% 76% Majority of stakeholders view IV morphine as likely to be replaced by OLINVYK:
Olinvyk.com Virtual “on demand” Medical Education programs HCP social media Professional Society Meetings & Congresses Field directed: live, virtual & email Omni - channel Approach for HCP Engagement 43 Communication across a full range of channels to maximize reach and impact Customize mix across channels
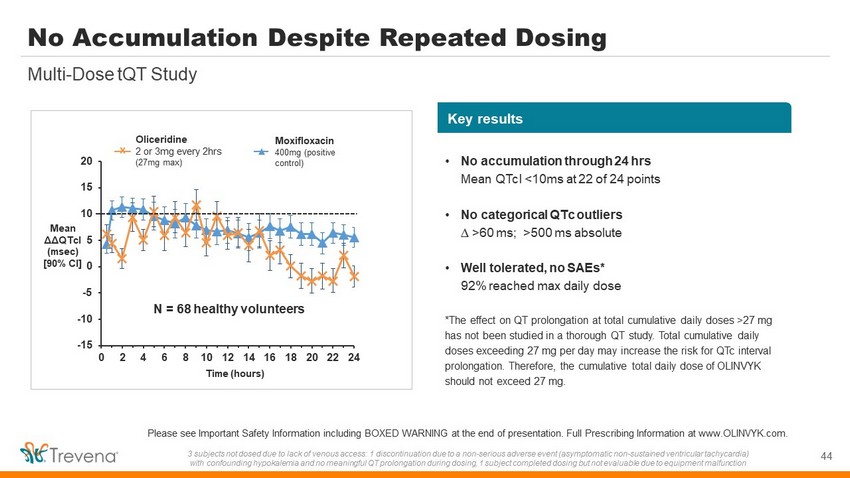
-15 -10 -5 0 5 10 15 20 0 2 4 6 8 10 12 14 16 18 20 22 24 Mean ΔΔ QTcI ( msec ) [90% CI] No Accumulation Despite Repeated Dosing 44 Multi - Dose tQT Study Please see Important Safety Information including BOXED WARNING at the end of presentation. Full Prescribing Information at w ww. OLINVYK.com. 3 subjects not dosed due to lack of venous access: 1 discontinuation due to a non - serious adverse event (asymptomatic non - sustai ned ventricular tachycardia) with confounding hypokalemia and no meaningful QT prolongation during dosing, 1 subject completed dosing but not evaluable du e t o equipment malfunction Oliceridine 2 or 3mg every 2hrs (27mg max) x Moxifloxacin 400mg (positive control) Time (hours) N = 68 healthy volunteers Key results • No accumulation through 24 hrs Mean QTcI <10ms at 22 of 24 points • No categorical QTc outliers ∆ >60 ms ; >500 ms absolute • Well tolerated, no SAEs* 92% reached max daily dose *The effect on QT prolongation at total cumulative daily doses >27 mg has not been studied in a thorough QT study. Total cumulative daily doses exceeding 27 mg per day may increase the risk for QTc interval prolongation. Therefore, the cumulative total daily dose of OLINVYK should not exceed 27 mg.
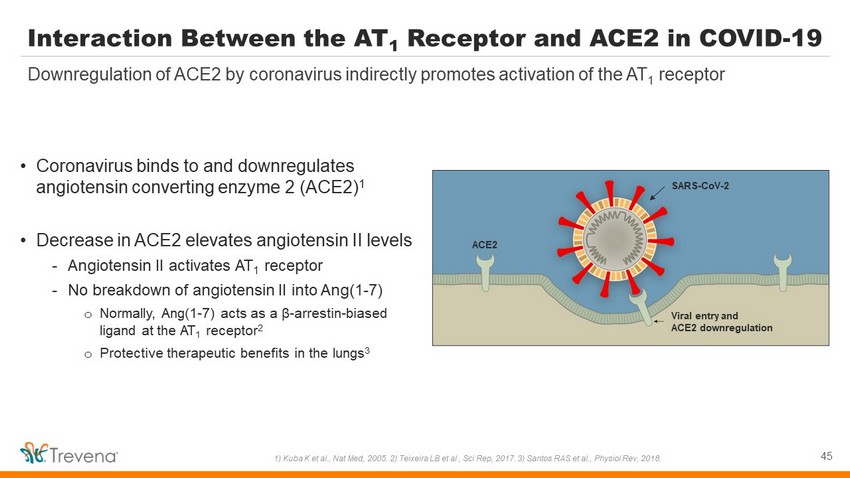
Interaction Between the AT 1 Receptor and ACE2 in COVID - 19 • Coronavirus binds to and downregulates angiotensin converting enzyme 2 (ACE2) 1 • Decrease in ACE2 elevates angiotensin II levels - Angiotensin II activates AT 1 receptor - No breakdown of angiotensin II into Ang(1 - 7) o Normally, Ang(1 - 7) acts as a β - arrestin - biased ligand at the AT 1 receptor 2 o Protective therapeutic benefits in the lungs 3 45 Downregulation of ACE2 by coronavirus indirectly promotes activation of the AT 1 receptor 1) Kuba K et al., Nat Med, 2005. 2) Teixeira LB et al., Sci Rep, 2017. 3) Santos RAS et al., Physiol Rev, 2018. SARS - CoV - 2 ACE2 Viral entry and ACE2 downregulation
TRV027 COVID - 19 Study - Imperial College London • Randomized, double - blind, placebo - controlled proof - of - concept study • N = ~60 (30 per arm) COVID - 19 patients - Hospitalized, non - ventilated - ≥18 years old • IV infusion of placebo or TRV027 for 7 days (12 mg/ hr ) • Review of interim data by DMSC found no safety concerns and supported advancement to more extensive study with clinical efficacy outcomes 46 Interim review by DMSC supports transition to REMAP - CAP trial DMSC = Data Monitoring & Safety Committee; 1) Primary endpoint: D - dimer levels. https://clinicaltrials.gov/ct2/show/record/NCT04 419610. ICL winding down s tudy ( Transition to REMAP - CAP) Primary ICL e ndpoint : Reduction of abnormal clotting associated with COVID - 19 1

Delta Receptor Agonists Have Unique Benefits Triptans / Ditans • Target: serotonin receptors mediate vascular excitability (a ssociated CV risk) 1 • Migraine - specific treatment CGRPs • Target: CGRP receptors regulate neuronal structures involved in pain signaling 2 • Migraine - specific treatment Delta receptor agonists • Target: delta receptors located in pain pathways; also distributed throughout brain regions associated with sensory information, emotional processing, and reward / impulsivity 3 • Potential for broad therapeutic application 47 Potential utility for a variety of CNS indications 1) Rothrock JF & Friedman DI, American Headache Society website: https://americanheadachesociety.org/wp - content/uploads/2018/05/ John_Rothrock_and_Deborah_Friedman_ - _Triptans.pdf. 2) Durham PL, Headache, 2006. 3) Peppin JF & Raffa RB, Journal of Clinical Pharmacy and Therapeutics, 2015.

IMPORTANT SAFETY INFORMATION 48

WARNING: ADDICTION, ABUSE, AND MISUSE; LIFE - THREATENING RESPIRATORY DEPRESSION; NEONATAL OPIOID WITHDRAWAL SYNDROME; and RISKS FROM CONCOMITANT USE WITH BENZODIAZEPINES OR OTHER CENTRAL NERVOUS SYSTEM (CNS) DEPRESSANTS Addiction, Abuse, and Misuse OLINVYK exposes patients and other users to the risks of opioid addiction, abuse, and misuse, which can lead to overdose and death. Assess each patient’s risk before prescribing OLINVYK, and monitor all patients regularly for the development of behaviors or conditions. Life - Threatening Respiratory Depression Serious, life - threatening, or fatal respiratory depression may occur with use of OLINVYK. Monitor for respiratory depression, especially during initiation of OLINVYK or following a dose increase. Neonatal Opioid Withdrawal Syndrome Prolonged use of OLINVYK during pregnancy can result in neonatal opioid withdrawal syndrome, which may be life - threatening if not recognized and treated, and requires management according to protocols developed by neonatology experts. If opioid use is required for a prolonged period in a pregnant woman, advise the patient of the risk of neonatal opioid withdrawal syndrome and ensure that appropriate treatment will be available. Risk From Concomitant Use With Benzodiazepines or Other CNS Depressants Concomitant use of opioids with benzodiazepines or other CNS depressants, including alcohol, may result in profound sedation, respiratory depression, coma, and death. Reserve concomitant prescribing for use in patients for whom alternative treatment options are inadequate; limit dosages and durations to the minimum required; and follow patients for signs and symptoms of respiratory depression and sedation. Limitations of Use Because of the risks of addiction, abuse, and misuse with opioids, even at recommended doses, reserve OLINVYK for use in patients for whom alternative treatment options [e.g., non - opioid analgesics or opioid combination products]: • Have not been tolerated, or are not expected to be tolerated • Have not provided adequate analgesia, or are not expected to provide adequate analgesia. The cumulative total daily dose should not exceed 27 mg, as total daily doses greater than 27 mg may increase the risk for QTc interval prolongation. CONTRAINDICATIONS OLINVYK is contraindicated in patients with: Significant respiratory depression Acute or severe bronchial asthma in an unmonitored setting or in the absence of resuscitative equipment Known or suspected gastrointestinal obstruction, including paralytic ileus Known hypersensitivity to oliceridine (e.g., anaphylaxis) WARNINGS AND PRECAUTIONS OLINVYK contains oliceridine, a Schedule II controlled substance, that exposes users to the risks of addiction, abuse, and misuse. Although the risk of addiction in any individual is unknown, it can occur in patients appropriately prescribed OLINVYK. Assess risk, counsel, and monitor all patients receiving opioids. Serious, life - threatening respiratory depression has been reported with the use of opioids, even when used as recommended, especially in patients with chronic pulmonary disease, or in elderly, cachectic and debilitated patients. The risk is greatest during initiation of OLINVYK therapy, following a dose increase, or when used with other drugs that depress respiration. Proper dosing of OLINVYK is essential, especially when converting patients from another opioid product to avoid overdose. Management of respiratory depression may include close observation, supportive measures, and use of opioid antagonists, depending on the patient’s clinical status. Opioids can cause sleep - related breathing disorders including central sleep apnea (CSA) and sleep - related hypoxemia with risk increasing in a dose - dependent fashion. In patients who present with CSA, consider decreasing the dose of opioid using best practices for opioid taper. INDICATIONS AND USAGE OLINVYK is a new chemical entity indicated in adults for the management of acute pain severe enough to require an intravenous opioid analgesic and for whom alternative treatments are inadequate. 49
WARNINGS AND PRECAUTIONS Prolonged use of opioids during pregnancy can result in withdrawal in the neonate that may be life - threatening. Observe newborns for signs of neonatal opioid withdrawal syndrome and manage accordingly. Advise pregnant women using OLINVYK for a prolonged period of the risk of neonatal opioid withdrawal syndrome and ensure that appropriate treatment will be available. P r o f ound s e d a tion, re spi r a to r y d e p r e ssion, c om a , a nd d ea th m a y re sult f r om the c on c omit a nt use of OLINVYK with b e n z odi a z e pin e s or oth e r C NS d e p re ss a nts ( e . g ., non - b e n z odi a z e pine s e d a tiv e s/ h y pnoti c s, a n x i o l y ti c s, t ra nquili z er s, mus c le re l a x a nts, g e n e ra l a n e sth e ti c s, a ntip s y c hoti c s, oth e r opioids, or a l c ohol ) . B e ca u s e o f th e se r isks, re s er ve c o n c omit a nt p re s cr ibi n g of th e se d r u g s f o r use in p a ti e nts f or whom a lt er n a tive t rea tm e nt options a r e in a d e qu a t e , prescribe the lowest effective dose, and minimize the duration. OLINVYK was shown to have mild QTc interval prolongation in thorough QT studies where patients were dosed up to 27 mg. Total cumulative daily doses exceeding 27 mg per day were not studied and may increase the risk for QTc interval prolongation. Therefore, the cumulative total daily dose of OLINVYK should not exceed 27 mg. Increased plasma concentrations of OLINVYK may occur in patients with decreased Cytochrome P450 (CYP) 2D6 function or normal metabolizers taking moderate or strong CYP2D6 inhibitors ; also in patients taking a moderate or strong CYP3A4 inhibitor, in patients with decreased CYP2D6 function who are also receiving a moderate or strong CYP3A4 inhibitor, or with discontinuation of a CYP3A4 inducer. These patients may require less frequent dosing and should be closely monitored for respiratory depression and sedation at frequent intervals. Concomitant use of OLINVYK with CYP3A4 inducers or discontinuation of a moderate or strong CYP3A4 inhibitor can lower the expected concentration, which may decrease efficacy, and may require supplemental doses. Cases of adrenal insufficiency have been reported with opioid use (usually greater than one month). Presentation and symptoms may be nonspecific and include nausea, vomiting, anorexia, fatigue, weakness, dizziness, and low blood pressure. If confirmed, treat with physiologic replacement doses of corticosteroids and wean patient from the opioid. OLINVYK m a y ca u s e s e v e r e h y po t e ns i o n, i n c l u d i n g or t h o s tatic h y po t e ns i o n a n d s yn c op e in a m b u lat o r y p atie n t s . T h e r e is i n c r ea s ed r i s k in p ati e n ts w ho s e a b ili t y to m a i n ta i n b l oo d pr e ssu r e h as a l r ea d y b een c o m pr o m i s ed b y a r e d u ced b l oo d v o l u m e o r c o n c u rr e n t a d m i n i s t r ati o n o f c e r tain C N S d e pr e ss a n t dru g s ( e . g . , phenothiazines or g e n e r al a n e s t h eti c s ). M o n it o r t h e s e p atie n ts f o r s i g n s o f h y po t e ns i o n. I n p atie n t s w i t h ci r c u lat o r y s h o c k , avoid the use of OLINVYK as it m a y c a us e v a s od ilati o n t h at can f u r t h er r e d u ce ca rd iac o u t p u t a n d b l oo d pr e ssu r e. A v o id t h e us e o f OLINVYK in p atie n ts w i th i m p ai r ed c o ns ci o u s n e s s o r c o m a. OLINVYK should be used with caution in p atie n ts w h o m a y b e s us ce p ti b le to t h e i n t r ac r a n ial e f f ec t s o f C O 2 r et e n ti o n, such as t h o s e with e v i d e n ce o f i n c r ea s ed i n t r ac r a n ial pr e s su r e o r br ain t u m or s , as a reduction in r e s p i r at or y dr i v e a n d t h e r e su lt a n t C O 2 r et e n ti o n can f u r t h er i n c r ea s e i n t r ac r a n i al pr e ssu r e. Mo n it o r su c h p at i e n ts f o r s i g n s o f s e d ati o n a n d r e s p i r at or y d e pr e ss i o n , p a r tic u la r l y w h en i n i t iat i n g t h e r a p y. As with all opioids, OLINVYK m a y ca u s e s p a s m o f t h e s p h i n c ter o f O dd i, and m a y ca us e i n c r ea s es i n s e r u m a my la s e. Mo n it o r p atie n ts w i t h b ilia r y t r act d i s ea s e, i n c l u d i n g a c u te p a n c r eatit i s , f o r w o r s e n i n g s y m p t o ms . T h e r e is i n c r ea s ed r i s k in p ati e n ts w ho s e a b ili t y to m a i n ta i n b l oo d pr e ssu r e h as a l r ea d y b een c o m pr o m i s ed b y a r e d u ced b l oo d v o l u m e o r c o n c u rr e n t a d m i n i s t r ati o n o f c e r tain C N S d e pr e ss a n t dru g s ( e . g . , phenothiazines or g e n e r al a n e s t h eti c s ). M o n it o r t h e s e p atie n ts f o r s i g n s o f h y po t e ns i o n. I n p atie n t s w i t h ci r c u lat o r y s h o c k , avoid the use of OLINVYK as it m a y c a us e v a s od ilati o n t h at can f u r t h er r e d u ce ca rd iac o u t p u t a n d b l oo d pr e ssu r e. A v o id t h e us e o f OLINVYK in p atie n ts w i th i m p ai r ed c o ns ci o u s n e s s o r c o m a. OLINVYK should be used with caution in p atie n ts w h o m a y b e s us ce p ti b le to t h e i n t r ac r a n ial e f f ec t s o f C O 2 r et e n ti o n, such as t h o s e with e v i d e n ce o f i n c r ea s ed i n t r ac r a n ial pr e s su r e o r br ain t u m or s , as a reduction in r e s p i r at or y dr i v e a n d t h e r e su lt a n t C O 2 r et e n ti o n can f u r t h er i n c r ea s e i n t r ac r a n i al pr e ssu r e. Mo n it o r su c h p at i e n ts f o r s i g n s o f s e d ati o n a n d r e s p i r at or y d e pr e ss i o n , p a r tic u la r l y w h en i n i t iat i n g t h e r a p y. As with all opioids, OLINVYK m a y ca u s e s p a s m o f t h e s p h i n c ter o f O dd i, and m a y ca us e i n c r ea s es i n s e r u m a my la s e. Mo n it o r p atie n ts w i t h b ilia r y t r act d i s ea s e, i n c l u d i n g a c u te p a n c r eatit i s , f o r w o r s e n i n g s y m p t o ms . OLINVYK m a y i n c r ea s e t h e f r e q u e n c y o f s ei z u r es i n p atie n t s w i t h s eiz u r e d i s ord e r s a n d may increase t h e r i s k o f s ei z u r es in vulnerable patients . M o n it o r p atie n ts w i th a h i s t o r y o f s ei z u r e d i s ord e r s f o r w or s e n ed s eiz u r e c o n t ro l. Do not abruptly discontinue OLINVYK in a patient physically dependent on opioids. Gradually taper the dosage to avoid a withdrawal syndrome and return of pain. Avoid the use of mixed agonist/antagonist (e.g., pentazocine, nalbuphine, and butorphanol) or partial agonist (e.g., buprenorphine) analgesics in patients who are receiving OLINVYK, as they may reduce the analgesic effect and/or precipitate withdrawal symptoms. OLINVYK may impair the mental or physical abilities needed to perform potentially hazardous activities such as driving a car or operating machinery. Although self - administration of opioids by patient - controlled analgesia (PCA) may allow each patient to individually titrate to an acceptable level of analgesia, PCA administration has resulted in adverse outcomes and episodes of respiratory depression. Health care providers and family members monitoring patients receiving PCA analgesia should be instructed in the need for appropriate monitoring for excessive sedation, respiratory depression, or other adverse effects of opioid medications. ADVERSE REACTIONS Adverse reactions are described in greater detail in the Prescribing Information. The most common (incidence ≥10%) adverse reactions in Phase 3 controlled clinical trials were nausea, vomiting, dizziness, headache, constipation, pruritus, and hypoxia. 50